
The below studies show that it’s possible the clavicle may grow past epiphyseal(growth plate fusion). However, the studies are limited in that the only go to 25. However, the slow rate of growth is indicative of a non-growth plate based method of growth as growth plate growth is typically much faster.
The Clavicle Continues to Grow During Adolescence and Early Adulthood
“As more adults undergo surgical fixation of clavicle fractures with improved outcomes, interest is renewed in managing clavicle fractures in adolescents. The medial clavicular physis does not fuse until 23 to 25 years of age{they think this but if you actually look at the study, clavicular growth does not actually stop at age 25}, but studies report minimal clavicular growth during adolescence—studies that employed cross-sectional methodologies, which cannot not capture growth in patients over time. The assumption that clavicle length at each stage is uniform, as is the final overall length, may not be accurate if the age groups studied comprise various ethnicities, socioeconomic status, or height.
We sought to quantify longitudinal clavicular growth on serial radiographs in adolescents and young adults. Our hypothesis was that substantial clavicular growth would be seen beyond the age of 12 years.
We conducted a longitudinal case series of non-syndromic patients in a single orthopedic clinic and analyzed serial radiographic images of the clavicles. For ethical reasons, only patients with non-neuromuscular scoliosis and kyphosis (in whom the existing standard of care includes serial thoracic radiographs) were considered for inclusion. Patients ages 10 to 25 years old were included in the study if three or more serial thoracic radiographs over a minimum 5 years were available that captured the entire length of at least one non-rotated clavicle. Three types of radiographs were included for analysis: digital low-dose-radiation stereoradiographic (EOS Imaging, Paris, France), non-EOS digital, and non-EOS printed. The overall longitudinal growth, yearly growth, and the yearly growth percentage were calculated for each clavicle.
Fifty-seven patients (22 male and 35 female) met the inclusion criteria. In male patients, at ages 12 to 15 years, the clavicular growth was 4.9 mm/year, or 4%/year; at ages 16 to 19 years, growth was 3.2 mm/year, or 2.4%/year; and at ages 20 to 25 years, growth was 1.7 mm/year, or 1.1%/year. In female patients, at ages 12 to 15 years, growth was 4.7 mm/year, or 4%/year; at 16 to 19 years, growth was 2.2 mm/year, or 1.7%/year; and at ages 20 to 25 years, growth was 0.2 mm/year or 0.1%/year{this incredibly slow growth rate is atypical of longitudinal bone growth based on the growth plate and I believe is indicative that the clavicle continues to grow into adulthood via non-growth plate based methods}. We could not detect the age of terminal growth in either sex because growth was ongoing in most patients in the oldest group.
We found substantial clavicular growth potential after age 18 years, when growth is thought to be nearly finished, as well as remodeling potential even up to age 25 years. Further research is needed, but our findings suggest that strategies for managing clavicle fracture in adults may not be applied universally to adolescents and young adults.”
“Our study is unique in that it demonstrates continued longitudinal clavicular growth beyond 18 years of age in both sexes. There was as much as 10% more growth after the age of 18 years in male subjects and as much as 6% in female subjects.”
I sent an email to the authors to see if we can see if there’s a possibility that the longitudinal bone growth does not occur solely based on the growth plate.
Clavicles continue to grow beyond skeletal maturity: radiographic analysis of clavicle length in adolescents and young adults
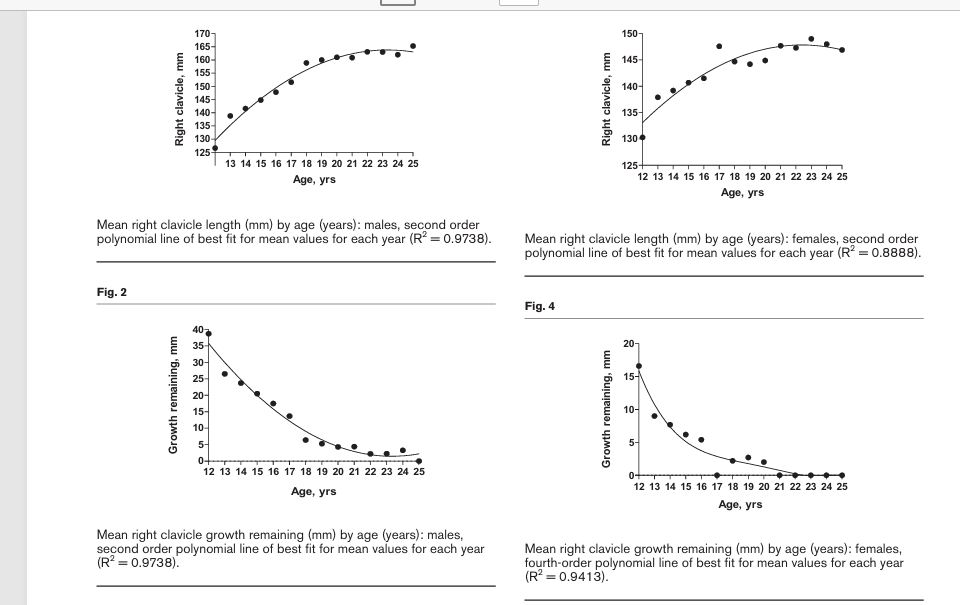
“There has been minimal research regarding the clavicle’s growth and its clinical implications in the late adolescent and early adult population. Previous studies have evaluated postnatal clavicle growth to age 18 without analysing growth through the age of secondary ossification center closure. The purpose of this study was (1) to determine clavicle length and age-related growth in males and females from age 12 to 25 years and (2) to specifically analyse clavicle growth in late adolescence. This was a retrospective analysis of chest radiographs in patients aged 12-25 years. The ruler tool was used to measure clavicle length. Mean values were tabulated for each year of age in males (n = 697) and females (n = 672). Mean right clavicle growth significantly increased from age 12 to 25 in both males and females (P < 0.0001). In males, the increase from age 16 to 25 was 17.5 mm, representing 10.6% of total clavicle length (P < 0.0001). In females, the increase from age 14 to 25 was 7.7 mm, representing 5.2% of total clavicle length (P < 0.0001). We found that from skeletal maturity to the closure of the secondary ossification center, growth was 17.5 mm (10.6% of total clavicle length) in males and 7.7 mm (5.2% of total clavicle length) in females. During their growth spurts, the adolescent male and female clavicle have growth potentials very similar to previous studies of radius growth. Understanding these clavicular growth potentials can influence operative vs. nonoperative management decisions by orthopaedic surgeons. Level of evidence: Level III.”
This description unlike the other other one does not suggest that growth can occur post closure of the secondary ossification center.
The graphs below although small suggest that it’s possible that small amounts of growth can occur between 20 and 25
This study is not as promising in turns of longitudinal bone growth post epiphyseal fusion but it does not rule it out either.
What we would need to do is look at clavical length past age 25 to see if there’s continued changes but I do not see any papers that study that. If we can prove that the clavical continues growing than we have another bone as proof of concept that longitudinal bone growth can occur past skeletal maturity.