
 In the previous post, I wanted to establish the basis for the origin of the idea for this question to see if we can somehow use the microfracture surgery technology to increase height. From a post, Tyler had said…
In the previous post, I wanted to establish the basis for the origin of the idea for this question to see if we can somehow use the microfracture surgery technology to increase height. From a post, Tyler had said…
“Scientists have utilized the power of microscopic fractures in stem cells with knee microfracture surgery to stimulate cartilage growth. You can also cause microscopic fractures in the ends of the long bones to release these powerful red bone marrow stem cells. Laterally pressing against the ends of your bones also increases fluid flow within the bone. This increase in fluid flow sends the stem cells to your now opened growth plate!”
The idea is theoretically sound and might work from a quick analysis. I would do a little more research on microfracture surgery. Let’s first see what Wikipedia says with it’s article on Microfracture Surgery. From Wikipedia…
Microfracture surgery is an articular cartilage repair surgical technique that works by creating tiny fractures in the underlying bone. This causes new cartilage to develop from a so-called super-clot. Microfracture surgery has gained popularity in sports in recent years; numerous professional athletes including …. have undergone the procedure.
The surgery is quick (typically lasting between 30-90 minutes), minimally invasive, and can have a significantly shorter recovery time than an arthroplasty (knee replacement).
Background
Chronic articular cartilage defects do not heal spontaneously. However, acute traumatic osteochondral lesions or surgically created lesions extending into subchondral bone, e.g. by Pridie drilling, spongialization abrasion or microfracture causing the release of pluripotent mesenchymal stem cells from the bone marrow, may heal with repair tissue consisting of fibrous tissue, fibrocartilage or hyaline-like cartilage. The quality of the repair tissue after these “bone marrow stimulating techniques” depends on various factors including the species and age of the individual, the size and localization of the articular cartilage defect, the surgical technique, e.g., how the subchondral bone plate is treated, and the postoperative rehabilitation protocol.
Procedure
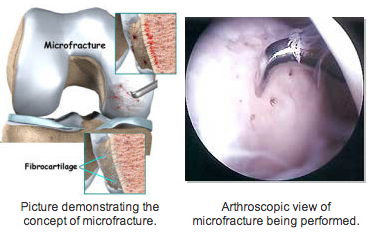
The surgery is performed by arthroscopy, after the joint is cleaned of calcified cartilage. Through use of an awl, the surgeon creates tiny fractures in the subchondral bone plate. Blood and bone marrow (which contains stem cells) seep out of the fractures, creating a blood clot that releases cartilage-building cells. The microfractures are treated as an injury by the body, which is why the surgery results in new, replacement cartilage. The procedure is less effective in treating older patients, overweight patients, or a cartilage lesion larger than 2.5 cm. Further on, chances are high that after only 1 or 2 years of the surgery symptoms start to return as the fibrocartilage wears away, forcing the patient to reengage in articular cartilage repair.
The effectiveness of cartilage growth after microfracture surgery is thought to be dependent on the patient’s bone marrow stem cell population and some think increasing the number of stem cells increases the chances of success. A couple of physicians are promoting an alternative treatment implanting autologous mesenchymal stem cells directly into the cartilage defect, without having to penetrate the subchondral bone.
Microfracture Reports
Studies have shown that microfracture techniques do not fill in the chondral defect fully, forming fibrocartilage rather than hyaline cartilage. Fibrocartilage is not as mechanically sound as hyaline cartilage; it is much denser and unable to withstand the demands of everyday activities as well as the original cartilage and is thus at higher risk of breaking down. The blood clot is very delicate after surgery and needs to be protected. In terms of time, the clot takes about 8 weeks to 15 weeks convert to fibrous tissue and is usually fibrocartilage by about four months post surgery, holding implications for the rehabilitation.
Chondrocyte Implantation procedures (CCI), a cell based articular cartilage repair procedure that aims to provide complete hyaline repair tissues for articular cartilage repair, have been posed by some as an alternative to microfracture surgery. In February 2008, Saris et. al published a large-scale study claiming that CCI results in better structural repair for symptomatic cartilage defects of the knee than microfracture surgery. According to the study, one year after treatment, the tissue regenerate associated with CCI is of better quality than that of microfracture surgery.
So we know a few things just from a Wikipedia article. This idea of purposely creating microfractures in the knee subchondral bone plate area in the shape of small circular holes will cause blood and bone marrow to flow out, cause some clotting, which will cause cartilage formation. It seems that the clotting action of the bone marrow with the stem cells inside which seeps out is what causes cartilage formation. The problem seems to be that the cartilage formed is fibrocartilage, NOT hyaline cartilage. We must remember that there are different kinds of cartilage. The growth plates and the articular cartilage are hyaline cartilage, which is what we are looking for and to create. However the idea of making very small microfractures and punctures through the bone into the subchondral layer is enticing. Cartilage is formed so that is a start.
From a section of the website for the US National Library of Medicine, National Institutes of Health…
Knee microfracture surgery
Knee microfracture surgery is a common procedure used to repair damaged knee cartilage. Cartilage is the material that helps cushion and cover the area where bones meet in the joints.
Description
Three different types of anesthesia may be used for knee arthroscopy surgery:
- Medicine to relax you, and numbing the knee using shots of pain killers
- Spinal (regional) anesthesia
- General anesthesia, where you will be asleep and pain-free.
The surgeon will make a 1/4-inch surgical cut (incision) on your knee.
- A long, thin device called an arthroscope is placed through this cut. It is like a camera. It is attached to a video monitor in the operating room. This tool allows the surgeon to look inside your knee area and work directly on the joint. See also: Knee arthroscopy
- The surgeon makes another surgical cut and passes tools through this opening. A small pointed tool called an awl is used to make very small holes, called microfractures (tiny breaks), in the bone near the damaged cartilage.
- These holes release cells in your bones that build new cartilage. Your body will build new cartilage to replace the damaged cartilage.
Why the Procedure is Performed
Your doctor may recommend this procedure if you have some damage to the cartilage in the knee joint and on the underside of the kneecap.
The goal of this surgery is to prevent or slow further damage to the cartilage, preventing knee arthritis. It can help you avoid the need for a partial or total knee replacement.
This procedure is also used to treat knee pain due to cartilage injuries.
Another surgery, autologous chondrocyte implantation, is done for similar reasons.
What we see from this resource is overall a repeat of the same information. From the website for the London Knee Clinic, it would seem that the procedure is similar in effect as the Autologous Chondrocyte Implantation (aka Transplantation). It says that in the beginning, there will be 1/4th of an inch in cut on the articular cartilage surface area. There is a 2nd cut and surgical tools are passed through this opening. Something called an awl (sharp pointy device??) is used to make the small holes, which is what the microfractures are. The hole are big enough to release the cells from inside the bones to the outside where the cartilage covering is but small enough that bone healing from the clotting effect will be easy and will be relatively simple and noninvasive.
This is Part II in a 3 post series where I look at the potential idea on using the techniques and theories from microfracture surgery to possibly find a way to increase height.