
This post is one of the most controversial ideas I have been thinking about since it would require that the human body change in shape and physiology in a dramatic way. One of the basic ideas of innovation by business analysts is that the person who is trying to figure out how to think outside-of-the-box needs to question and challenge all assumptions to test to see if they are all valid. Well this post is going to challenge some of our most basic ideas on how endochondral ossification and how the structure and alignment of the growth plates to the bones might work.
When I was reading over on how the long bones are even formed in the beginning from chondrogenic condensation & aggregation, I started to wonder whether it might be possible to create more than just the primary and secondary ossification center as expected from the neonatal development of humans. I am proposing that if we had more than the usual 1 primary and 2 secondary ossification centers , but had an additional primary ossification center then we would have more than just the two growth plates on each side, proximal and distal, of each long bone in our limbs. We might be able to create 4 growth plates on each limb. So, an we create the long bone development to have two secondary ossification centers and two or even three primary ossification centers?
We know that humans naturally develop ‘growth plates’ because the specific areas when the cartilage tissue starts to ossify/turn into bone are pushing against each other, turning what used to be entirely made from cartilage tissue into a band of cartilage that is left. Cartilage can expand due to the elastic, deformable nature of the extracellular matrix composition. the cells in the matrix can expand and push against each other, which would cause the entire tissue to expand with the expansion of the cells.
 First, from basic anatomy, we have to realize that there is really no such thing as ‘growth plates’. The actual term for growth plates is just a name given to the band of cartilage that has not been encroached upon and turned into bone. I refer to picture to the right is taken from a class at Midlands Tech. The picture is small so it might be smart to click on the picture to make it bigger.
First, from basic anatomy, we have to realize that there is really no such thing as ‘growth plates’. The actual term for growth plates is just a name given to the band of cartilage that has not been encroached upon and turned into bone. I refer to picture to the right is taken from a class at Midlands Tech. The picture is small so it might be smart to click on the picture to make it bigger.
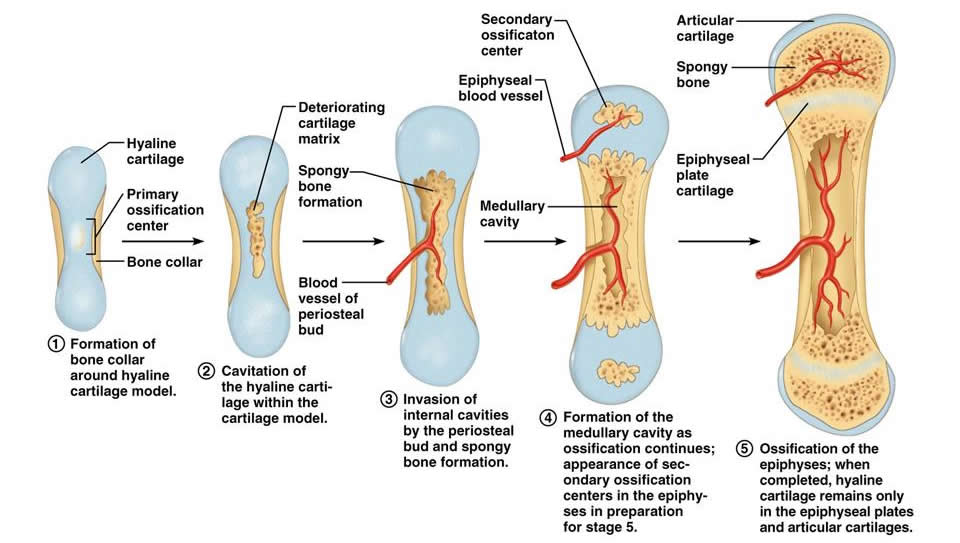
We see that in the actual development of the bones which grow not just longer but also wider, that the bones start out as completely cartilage, when the human is still in the womb and growing as an embryo. I don’t know enough about obstetrics but I would guess that the fetus starts to have some of the earliest cartilage tissue ossify before it is even born. If that was not the case and the long bones were still cartilage, from the process of birth where the fetus’s head has to pass through the birth canal, it’s cartilage head would be completely deformed or even crushed by the PC muscles of the female vulva region. Its body and limbs should also be partly bone or the mother and father in the hospital room would not be ale to hold the baby that was just born without hurting it through deformation of the cartilage.
Without reading anything on pediatrics or pediatrics growth, I am assuming right now that when the baby is just born, it already has the ends of the cartilage structure start to ossify and the diaphysis also ossify too. This is the beginning of where the ossification centers are.
So the growth plates are just where the ossification centers meet and where they haven’t encroached completely on through vascularization and mineralization.
I am proposing that it might be possible to have a limb bone growth with almost unlimited length if we can get a second band of cartilage alongside the original band of cartilage in the long bone’s bone tissue.
Depending on how the double growth plate would go together, and in which arrangement might be slightly tricky, at least at this stage. We know that the growth plates have around 4 basic zones which must all function in continuous, sequential path.
- Resting Zone – where the progenitor mesenchymal stem cells differentiate into the chondrocytes
- Proliferation Zone – the area where the cartilage cells multiply through the process of mitosis
- Hypertrophic Zone – the area where the actual bone lengthening (or actually cartilage matrix expansion) is being done.
- Calcification Zone – the area that is being infiltrated, vascularized, and mineralized to turn the cartilage tissue matrix into bone tissue matrix
The smooth sequential series of cell differentiation steps must also work for the 2nd growth plate, which would be implanted into the limb’s long bone, around the metaphyseal area, in parallel with the natural one.
The Actual Arrangment
I remember reading that the way that the cartilage/growth plate actually manage to make the overall bone structure longer is that while the middle part of the long bone stays where it is, there is a part of the bone that is slowly being PUSHED away from the other area/ distance of the overall bone structure. Technically, the epiphyseal ossification center, which is the secondary center is being pushed outward by the continuous cartilage into bone tissue process of calcification aka ossification.
So remember this part – The natural process of how long bones get longer is that the resting zone is actually pushing the long bone’s ends, the epiphysis away from the center of the long bone structure. From physics, we have to remember that there really is no such thing as a PULLING FORCE. Anything that is moving is the result of a force that is doing PUSHING, NOT PULLING.
So what surface of tissue is pushing which surface of tissue to make the long bone longer?
The general current medical conclusion is that the edge of the growth plate that is on the epiphysis side (aka the resting zone side) is pushing distally the epiphysis away from the spatial center of the bone.
So how does this relate to the principle of height increase through double growth plate implants?
We have to decide in which direction should the growth plate go in, with either the resting zone facing outwards from the center of the bone, or facing inwards towards the center of the bone. Remember that the natural growth plate is facing away from the medium.
The 2nd thing to remember is that there has to be a continuous source of bone marrow derived mesenchyme that can differentiate into the cartilage cells/chondrocytes that we want. If we put the growth plate in the wrong direction, the bone marrows progenitor mesenchymal stem cells might not be enough and get depleted.
I present a picture found elsewhere below.
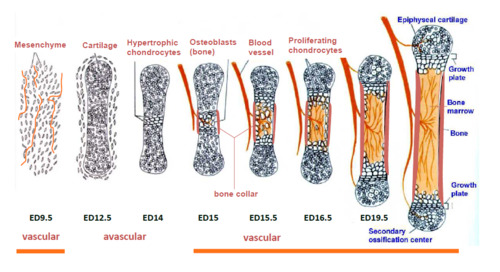
Notice that the blood vessels are going in only certain parts of the long bone so that the organic tissue in the cavity in the middle is kept alive. This would be the same blood vessel which would continue to make new progenitor mesenchyme. While there is maybe one major vessel going into the epiphysis, there is much more going into the middle of the bone. That is why I propose that the direction which a 2nd growth plate on each side should be put in be facing the direction where the resting zone would be on the side closer to the middle. The result is an overall long bone that actually has 5 sections, instead of the usual 3 sections, which results in 4 growth plates on each limb.
Complications With This Idea
The main issue with this proposal is from the failure of the long bone’s structural integrity because it became too long and the body became too heavy. The loading on the continuous cartilagenous area from above the growth plate would get heavier and heavier as the person got older, and the cartilage may not longer be able to support the body. If the bone, like a femur, became too long, it might become too weak