Electromagnetic Stimuli Will Increase Ossification and Make Bones Longer, Big Breakthrough!
 Note #1: I will be doing a podcast episode specifically about this post because it is so influential. There will be a lot of name dropping (sorry about that) and for all of you guys out there doing serious research just like me and Tyler, help out the cause and look into the links and studies which I will link below. I am just one person and research all of the leads. In some ways we ARE detective, trying to piece together puzzles to figure out what all of the data and study results actually mean. You can check out all of the older podcast episodes by CLICKING HERE!
Note #1: I will be doing a podcast episode specifically about this post because it is so influential. There will be a lot of name dropping (sorry about that) and for all of you guys out there doing serious research just like me and Tyler, help out the cause and look into the links and studies which I will link below. I am just one person and research all of the leads. In some ways we ARE detective, trying to piece together puzzles to figure out what all of the data and study results actually mean. You can check out all of the older podcast episodes by CLICKING HERE!
Note #2: There is actually a section on Biological Immortality in this post. I will go into a little bit of detail on that as well to show that in my own quest to figure out how to grow taller, I might have also accidentally stumbled upon another interesting scientific endeavor, which is to figure out the mechanisms on how biological immortality is possible..
Articles like this don’t come every day, and this post I feel will be one of the most important posts I have ever written for the website, if not the biggest in terms of breakthroughs, because this is huge. The only other article that comes close might be the study where I showed that synthetic human epiphyseal cartilage had already been created more than a decade ago
 Recently I finished reading the book The Body Electric by the late Dr. Robert O. Becker. (You can get the PDF for the book just by clicking the link above which is around 21 MB) In the book Dr. Becker talked about how he would be able to stimulate lower level forms of organisms, specifically salamanders to regenerate entire limbs.
Recently I finished reading the book The Body Electric by the late Dr. Robert O. Becker. (You can get the PDF for the book just by clicking the link above which is around 21 MB) In the book Dr. Becker talked about how he would be able to stimulate lower level forms of organisms, specifically salamanders to regenerate entire limbs.
I also managed to upload for you guys to download the PDF for the book Electromagnetism and Life written by Dr. Becker and his assistant at the time Andrew Marino. Click the link above to download.
So the Beginning of this post Starts 3 Days Ago…
At the end of Dr. Becker’s seminal book, his tone turns angry as various government agencies and departments try to shut down his lab and his research. Something that is not well known is that the primary job of a professor is NOT to teach, BUT TO DO RESEARCH. To do research you need to have the money to buy all the lab equipment. That is why one of the main jobs of professors is to write grants to government agencies begging for money.
Robert Becker started to make a lot of enemies back in those days. He was actually interviewed on 60 Minutes along with his assistant at the time, an assistant/post-doc named Andrew Marino. They talked on the interview about the harmful effects of EMFs, which is short for Electromagnetic Fields.
It turns out that back in the 1980s and early 90s Becker was getting a lot of press from his research on the harmful effects of EMFs. I personally remember that there was even a movie starring Eddie Murphy called The Dinstinguished Gentlemen where he plays a conman-turned-politician who goes to a small town to see young kids who developed Cancer from living so close to high power lines. That was big news 20s years ago.
 So I finished the ending of the book, and decided to track down this Dr. Marino. It turns out that almost immediately after Dr. Becker’s lab was disbanded by the various government agencies he was fighting against back in the 80s and early 90s, Dr. Marino went to Louisiana State University, and has been there for at least 20 years now. Currently he holds the titles of Professor & Director of Research @ the Division of Sleep Medicine, Department of Neurology, Department of Cellular Biology and Anatomy, Louisiana State University Health Sciences Center, Shreveport, LA. Click Here to get to his faculty profile on the LSU website.
So I finished the ending of the book, and decided to track down this Dr. Marino. It turns out that almost immediately after Dr. Becker’s lab was disbanded by the various government agencies he was fighting against back in the 80s and early 90s, Dr. Marino went to Louisiana State University, and has been there for at least 20 years now. Currently he holds the titles of Professor & Director of Research @ the Division of Sleep Medicine, Department of Neurology, Department of Cellular Biology and Anatomy, Louisiana State University Health Sciences Center, Shreveport, LA. Click Here to get to his faculty profile on the LSU website.
It seems that Dr. Marino actually writes his own blog and documents his personal thoughts. I found one of his older posts from back on Sept 9, 2011 (Click here to get to it) which was entitled “The 3 B’s and the Scientific Outlook“. The three B’s he is referring to are…
- Dr. Carl Brighton M.D, Ph. D. – I’ve talked extensively about him already. Still alive and only gave one email back in response, which was the first one. Never responded back to me ever again.
- Dr. Robert O. Becker M.D. – He is starting to become one of my scientific heros. He died fairly recently back in 2008. He was actually nominated for the Nobel Prize twice!
- Dr. C. Andrew L. Bassett M.D. – He was an orthopedic surgeon associated with Columbia University for a couple of decades. I tried to find him but found that he passed away back in 1994. Click here to read an article I found detailing his work and death
I clipped the cover of the the post for you guys to see. You can see what they looked like
So far I have only researched the work on Dr. Brighton and Dr. Becker. The reason why I have become almost obsessed with Dr. Becker’s work is because my 2nd Project, which I am focusing 90% of my energy on right now, is in doing research on the medical benefits of sending various types of electrical stimuli into the body.
Becker had evidence that it might be possible for humans to regenerate limbs from using DC current!
So I did two things…
I found the email to Dr. Marino on his website which is amarino@lsuhsc.edu – I emailed Dr. Marino and asked whether he is willing to come on the website and let me interview him on the research he was so passionate about two decades ago. The fact that he writes about Dr. Becker even almost 20 years after the lab and research shows that he obviously still cares a lot about the work. He has currently not emailed me back. If he says yes, I will record out interview and place it as a podcast episode. Woohoo!
I once said that if I could get Dr. Brighton on the podcast for an interview it would be the greatest coupe for the website and our research. Since he never responded back after the 1st response which he did give, I guess it is never meant to be. Within the “3 Bs” he is the only one who is still alive!
When he passes away, he will take all of the research and work with him. Of course I am talking about the unpublished works, the lab experiments which didn’t work. Those are the one which are probably more worth studying. We know from business and academic research that most of our ideas and hypothesis don’t work out. In academics, you only publish the success stories. Your failures and failed lab tests are almost never recorded. That type of information can only be obtained through interview and questioning.
I sort of realize that Dr. Marino is still angry at Brighton since Brighton promoted EMFs but Becker was very much against EMFs. Brighton & Bassett said that EMFs were completely safe but Becker cautioned about it since his groups’ research showed otherwise.
There was a 2nd blog post published in Sept 19, 2011 entitled “The 3 B’s and Electrical Stimulation of Bone Growth“. I also took the liberty of clipping the blog’s entry to show another picture of Bassett with Brighton.
So since Mr. Marino has not responded back even after 3 days, there was only thing I could do.
I started to do research on the type of work that Bassett worked on. What I found was astounding!!
In the previous post, which was just my usual monthly update, I had said that there is a guy named Kronberg which had figured out to make a device for bone growth, in terms of bone density increases. That device will cause increased ossification but the medical benefit is reduced chances for bone fracture and reversal of the onset of osteoporosis from old age.
What Dr. Andrew Bassett did was much more in depth. Just from one source alone, it captures what I have been suspect of for a long time. Using PEMF stimulation does absolutely work in bone growth, and NOT JUST IN TERMS OF BONE DENSITY, but has an effect on cartilage tissue/cells as well!
From the 1994 New York Times article documenting his passing from a brain tumor, I quote what was written & summarized about Dr. Bassett’s 20 years of work…
“In 1978, after 20 years of investigation and a five-year study of outpatients, he reported that electromagnetic waves could be used to heal fractured limbs. He developed devices that put to work the discovery that cell functions within the organism could be controlled by external electromagnetic fields….”
I looked on PubMed, and Google Patents, and other archives to see what Bassett had published and invented back in the 1980s.
Finding #1: Bassett founded two companies, Electro-Biology Inc and Osteodyne Inc.
Electro-Biology Inc was eventually bought out by BioMet back in 1988. The current medical devices sold is the EBI’s OsteoGen™ Bone Growth Stimulator. This is from Bassett’s research. Another model is the SpinalPak spine fusion stimulators. I actually wrote a review on the device in an older post from last year.
This hows that all of the bone growth and fracture healing devices that BioMet currently sells are all derived from Bassett’s work from 20 years ago.
Finding #2: When I used google to find information on Osteodyne Inc, the results showed certain patents Bassett had published.
- Method and device for treating bone disorders by applying preload and repetitive impacts – US 5484388 A
- Device for treating bone disorders – EP 0427732 B1
- Method and device for treating bone disorders – WO 1996003104 A1
- Method and device for treating bone disorders characterized by low bone mass – US 5046484 A
- Biomechanical-stimulation apparatus and method for bone regeneration – EP 2052708 A1
- Non-invasive method and means for in-vivo bone-growth stimulation – WO 1993024092 A1
Of course those above are just his patents. The list below are his studies and papers published which I found on Pubmed.
All of these studies showed that if you applied DC Current in a frequency and intensity of just a reasonable level (often about 1-30 Amps), the bones can be stimulated for increased ossification. Some of the titles of the studies give it away immediately.
It also seems like Bassett & Becker collaborated on a few papers together. Their research was just sending electrical signals to the bone in a lab animal in vivo.
This G. Cochran guy is someone that I realized collaborated extensively with Bassett
What we have to realize is that the internet was not available back in the 80s or early 90s for most people. Only people who were associated with DARPAnet and the Department of Defense knew anything at all about how computers and connections worked back then.
If anyone would have been doing research to figure out height increase back then, they did not have the types of resources which we have now. There was no way that a lay person, or amateur medical researcher would be able to find this type of information. Now in the year 2013 we as amateur scientific researchers can use the power of the internet, the WayBack Machine, Google Scholars, and Patent Records to find all of this type of information which might have been recorded even 50-60 years ago.
Note: A lot of these studies are referenced and mentioned in the physician handbook Development And Growth edited by Geoffrey Bourne. I would love to get a copy of that book to go over the literature of what is written on bone fracture healing techniques and compare what I have found with that book.
So the obvious question for anyone who has done any type of research would be…
How does this information help us grow taller?
The obvious rebuttable is would be this – while E&M field generation could make bone fractures and non-unions heal, that DOES NOT mean that the bones get longer. Remember, every single device or pill (like using statin derivatives) lead to bone density or bone mass increase, NOT volumetric increase where the bone gets longer!!
Bones sort of have natural tendency to heal. Bones are actually one of the only tissue in the human body that has regenerative abilities. If you cut the heart, the wound will not heal over. A Bone fracture does. That is what makes it so special compared to the other tissues in the human body.
Based on The Body Electric book, I have learned that the locations where the bones actually start to heal is from two main places…
- The intermedullary cavity, which stores the bone marrow in any long bone in the human skeletal system.
- The periosteum – It seems that you always want to keep the periosteum intact.
The cortical bone and cancellous bone part DOES NOT heal, but those two areas.
What we really want to do is get the cartilage tissue in the bones to start to expand. To do that, the two chondrocyte processes of proliferation & hypertrophy must go together.
So What Can the Average Person Do?
This is a proposal which I think would be a very revolutionary idea. A person would need the following items.
1. A set of acupuncture needles that have been covered in silver metal.
2. Cooper wiring cord to connect the needle to the power source.
3. The power source
4. A way to change the frequency and the intensity of the electrical current.
The first thing that would be needed are silver/metal needles, similar in shape and size to what you see what acupuncturists use.
Robert Becker in the book talks about his research into the TCM practice of acupuncture and stated that his theory was that the needles when used on various pressure points in the body had some type of effect on
The other big thing is that from the research of Becker (and the Physicist Bob Beck, inventor of the Beck Protocol) it was found that silver has some extremely positive effects on bone growth. If you attach a silver sheet over a bone wound which has some serious infection and send negative potential (from a DC source) through the copper wiring it is connected to, the silver has some type of anti-microbial effect. Silver promotes bone growth and kills microbes. Of course it has been known for thousands of years since the ancient Chinese and Greeks that wound infections seem to heal faster from silver contact. Seriously Guys, Read the Book!!
I say that the acupuncture needles need to be covered in a silver layer because there will be some invasive techniques involved. Becker used electrodes that were completely silver, but I am not sure where a normal person would ever be able to buy 100% silver acupuncture needles.
Power Source – As for the Power Source, most people including Bassett, Brighton, and Becker all promoted DC Current although I am still in the camp believing in AC. Maybe even an ordinary AAA battery with a 1.5 Volt might be enough. What I do know is that while Brighton and his lab assistants used 10,000-20,000 NanoAmps per centimeter of silver electrode to get a response from the bone tissue, Becker and his lab assistances got the same results using just 100-200 NanoAmps (per centimeter of electrode) emitted. As for the volts – It seems that beyond just 1 Volt, Brighton’s research found that the DC power source seemed to have some type of damage to the tissue. That was too much. That means that we might not need a device that needs more than just 1 regular AAA battery. However, we do have to talk about the resistors.
Here was Dr. Becker’s reasoning on why acupuncture worked, which I paraphrased from his words in the book…
He thought the acupuncture meridians were electrical conductors that carried injury messages to the brain. Any current grows weaker with distance, due to resistant along the transmission cable line. This is basic Electrical Engineering knowledge.
The smaller the Amp or Volts, the faster the current dies out. That is why EEs have built current amplifiers along the cable line, to bring the current back up. Becker thought that those “chi” points aka acupressure points or “ki” points were the body’s natural amplifiers which boosted up the signal of current flowing down a nerve which is slowly lost due to natural resistance. So basically an acupuncture point was in analog a DC Power source or booster. Becker got a new assistant with Maria Reichmanis, and they showed that the traditional chinese medicine meridian lines were indeed conducting current, and the polarity of the readings showed that for each acupuncture point was positive in polarity compared to the surrounding region. Each acupuncture point had their own electrical field being emitted. What was ultimately guessed by Becker was that the entire theory of acupuncture can be explained by the fact that the peri-neural cells were carrying current. That is what a metal needle stuck in would disrupt.
So the use of acupuncture needles will be three fold…
- They act as electrodes – we will connect them to a power source.
- They will be covered in silver, which is anti-microbial, and has bone generating abilities.
- They stimulate acupuncture points, which Becker seems to show are just peri-neural cells
What is a normal person supposed to do?
- Get the right type of silver electrode/ acupuncture needle.
- Find a normal conductive wire.
- Use a normal DC battery.
- Get an acupuncture chart – You want to get the dorsal region right above the SP9 point.
For proof that acupuncture works, read the PubMed study “Trigger point acupuncture for treatment of knee osteoarthritis“. They had used trigger point acupuncture therapy.
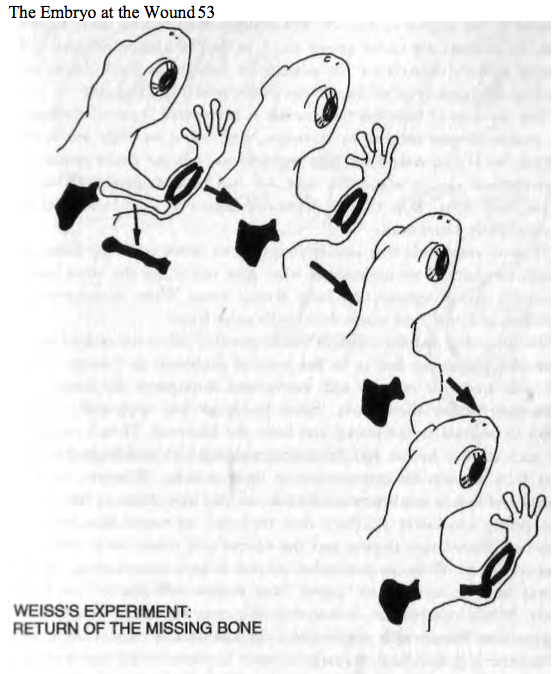
I personally would guess that what a person can start doing is first they stick the needle/electrode to just the area right above the epiphyseal plates. We found from a few old studies that if you cut a hole in the diaphysis of long bone and use an awl to cut apart the blood vessels, the longitudinal bone growth gets increased slightly. This is due to the fact that long bones have separate groups of blood vessels going to separate regions. There is a group of arteries going only to the epiphysis and another group supplying the blood to the diaphysis. What I am saying is that we want to get the electrodes to be close to the blood vessels supplying nutrients to the epiphysis only. Why that is the case we are not sure yet.
What about the Frequency and Intensity that we need to adjust for?
This part will need to be edited for later. There are a lot of values for frequency, duration of session, number of sessions per week, and intensity of the current, flying around in the various studies. I’ll edit this section when I organize everything.
I am extremely confident that this technique will result in increased longitudinal growth for the long bones for people will intact epiphyseal growth plates. For children who wish to be taller, this would be the most cost effective alternative that is possible.
Recently the company Biomarin has developed a drug known as BMN-111 which is supposed to treat dwarfism for children only (aka people still with growth plates) . You can read the article on the drug by clicking here. The way the drug works is through the stimulation of the CNP and through inhibition of the FGFR3 gene. We have already done research and understand the process of how CNP is stimulated through mTOR and Rapamyxin reasonably well. That treatment would cost over $50,000 for any parent who does not wish their kids to end up less than 5 feet tall. This I believe is a very reasonable alternative to Biomarin’s Dwarfism treatment, which would involve a lot of money.
Tyler has been promoting both the LIPUS and PEMF technology for years, but I personally think he has put more emphasize on the LIPUS method. From this post, I am trying to give conclusive proof that it would be much better to be focusing and promoting the PEMF path.
Further Validation of This Concept:
I refer to the Patent – Methods for modulating chondrocyte proliferation using pulsing electric fields – US 20080039901 A1
This patent was published back in 2008 by James Kronberg, who I have mentioned before. You can find the same patent from Google Patents. He used a pulse burst mode and continuous mode for the signal shape and duration. From the abstract he states that you can increase cartilage repair from stimulating NO production….
“…Cartilage, bone and other connective tissue growth is stimulated in part by nitric oxide release through electrical stimulation and may be modulated through co-administration of NO donors and NO synthase inhibitors. The methods and devices described are useful in promoting repair of bone fractures, cartilage and connective tissue repair as well as for engineering tissue for transplantation”
The other articles are…
The abstract of this paper almost states in plain english that using a PEMF of just low intensity would be enough to stimulate the process of endochondral ossification. You can get an increase in cartilage molecules, glycoaminoglycan content , and extracellular matrix production.
Million Dollar Question – Will It help a person with closed growth plate grow longer bones?
I suspect at this point that for people with closed growth plates, there is a slight probability, with maybe a 5-10% chance of it having some effect.
This is due to three related studies I did find.
- Effects of pulsed electromagnetic fields on human articular chondrocyte proliferation.
- Millicurrent stimulation of human articular chondrocytes cultivated in a collagen type-I gel and of human osteochondral explants.
- Effects of pulsed electromagnetic fields on articular hyaline cartilage: review of experimental and clinical studies
I showed in a recent post that there are still chondrocytes in the adult human articular cartilage in the ends of the epiphysis. The post was “Articular Cartilage At The End Of Epiphysis Do Growth Thicker Making Bones Longer (Big Breakthrough)”
This method would have some type of dramatic effect on the articular cartilage as well.
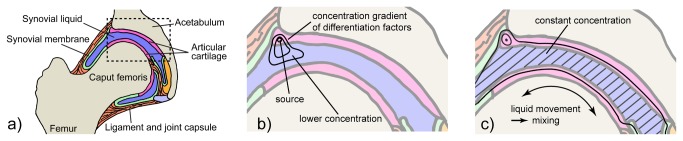
If we remember that way that the tissues layers are aligned next to each other underneath the cartilage layer, we realize that there is a subchondral layer. That layer can be thickened using the correct implantation location of the silver electrode to stimulate both an increase in the cartilage ECM and the increased deposition of the bone layer.
This part still needs to be edited further.
The section on biological immortality
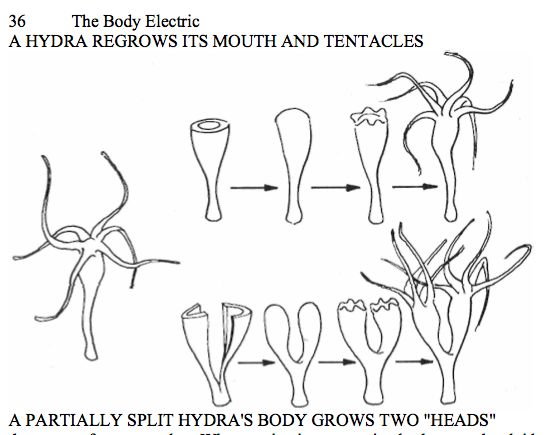
The finding was actually completely unexpected. In recent years, starting around the 2010-2011 time frame, there was a lot of articles published about this biologically immortal living organism called the Hydra. We suggest the study/paper “MORTALITY PATTERNS SUGGEST LACK OF SENESCENCE IN HYDRA“ or “Longevity Gene Makes Hydra Immortal and Humans Grow Older”
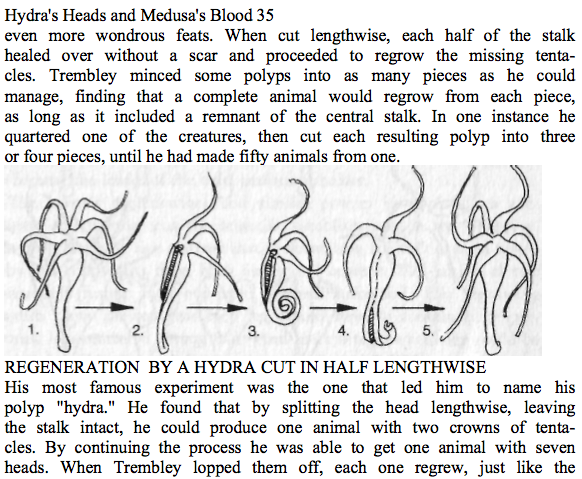
It would turn out that when I was reading up on Becker’s book that the Hydra was mentioned very early on. I took the chance to clip a picture of the Hydra which was from page 34 of the book.
A lot of the journalists who tried to cover the story and science on the Hydra seems to state that there is almost no research and information on the Hydra. Well they are wrong!
Becker and Abraham Trembley who lived 3 centuries were already studying this immortal creature. It seems that not only is the hydra biologically immortal, it might be completely immortal. Cutting the creature won’t kill it.
So not only can it live forever, it is almost nearly impossible to kill the creature even if you wanted to!!
It’s only weakness seems to be in the stalk. If the hydra cuts a leg or head off without the stalk, then it won’t regenerate. however if the head or leg cut off has any part of the stalk, the cut pieces will all eventually regenerate back into a whole intact body.
This is where the scientists right now who are studying why senescence seems to go in reverse for Hydra have not made the connection yet. There is even more to the Hydra that they realize.
What are the implications?
My research for this website was always towards height increase, the manipulating of tissue engineering, advanced electromagnetic stimuli, and such for a cosmetic gain. This finding I saw from reading over books written by researchers who have been criticized.
There has been a lot of talk in the medical community about the discovery of the FoxO Gene and that has sort of gotten people excited. The way that the Hydra reproduces is through budding. For further reading on the Hydra and immortality, read the article “Could this immortal hydra polyp inspire advanced rejuvenation therapies for humans?“