I was reviewing old LSJL papers and I found this nugget from “Diaphyseal bone formation in murine tibiae in response to knee loading”
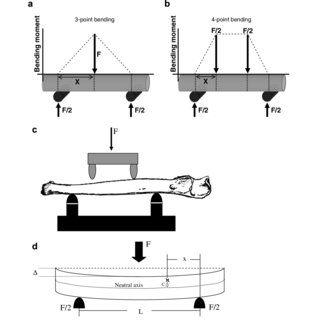
” conceivable hypothesis underlying these observations of bone formation with the knee-loading modality is that mechanical loads applied to the epiphysis induce the osteogenic signal towards the diaphysis through fluid flow in the lacunocanalicular network (1st model) or through alteration in blood circulation (2nd model)”
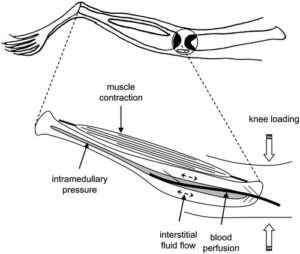
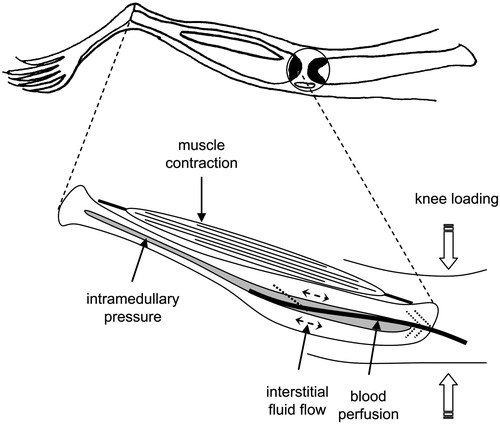
“Potential contributors to enhance bone formation in the tibia with knee loading. This schematic illustration includes muscle contraction, alteration in intramedullary pressure, load-driven interstitial fluid flow, and activation of blood perfusion.”
So these are all the methods to stimulate the bone. We want to find the method that stimulates interstitial fluid flow, blood perfusion, and intramedullary pressure the best to increase height. I believe that lateral impact loading is the best except it does not involve muscle contraction. The simple solution is to contract your muscle while performing lateral impact loading. The two most common methods of stimulating these forces muscular loading and axial impact are not enough to stimulate these forces above the threshold needed to increase height.
Here’s some more information about the fluid flow and intramedullary pressure.
Blood bone perfusion can be measured(Noninvasive methods of measuring bone blood perfusion) so it would be nice if we could test several different methods to see what generates the highest force.
FLUID MOVEMENT IN BONE: THEORETICAL AND EMPIRICAL
“Evidence from the literature and from our laboratory demonstrates a pronounced and rapid flow of fluids and associated solutes through the extravascular spaces in bone. Minutes after injection, large molecules such as ferritin and horseradish peroxidase (HRP) have been localized throughout the osteocytic lacunae and canaliculi of cortical bone in the chick, rat and dog. Patterns of marker movement preclude diffusion as the mechanism for solute movement and suggest a centrifugal bulk flow of fluids. We have developed a computer model of bone fluid flow that has led to the conclusion that the pattern and rate of fluid movement is governed by the pressure differential across the bone, the vascular architecture, and the porosity of the mineralized matrix. The validity of simulations in which a substance is injected and monitored over time has been tested by comparisons with actual injections of markers in the rat. Evidence is presented for a relationship between blood flow and bone dynamics in growth, repair and pathology of bone. We employed the tail suspension model of weightlessness in the rat to test the effect of posture on the perfusion of cortical bone using injections of HRP. Data indicated that perfusion of the femur was reduced by this treatment. We propose a “rheostat” mechanism, which suggests that bone perfusion may set limits for bone growth and remodeling. Therefore, bone mass reflects the ability of the vasculature to supply oxygen and nutrients to the cells on and within the mineralized matrix.”
“The blood supply to the long bones comes from three sources: the nutrient arteries. the periosteal arteries. and the metaphyseal-epiphyseal arteries”
The studies can go on and on. The point is that there is a threshold of forces:
- blood perfusion
- Intramedullary pressure
- Interstitial fluid flow
- Muscular contraction
Such that you can grow taller. I believe that the primary force is intramedullary pressure. LSJL(Knee loading) is primary deformations of the epiphysis which I don’t believe to be the best way to increase intramedullary pressure as it is indirect. The best way to increase intramedullary pressure is directly on the region itself. Thus lateral impact loading directly on the diaphysis.
Bodybuilders should already have high blood perfusion and muscular contraction so it is unlikely that those two forces can make you taller. Unless that threshold is really, really high.
Interstitial fluid flow unless it degrades bone is mostly about delivering nutrients to bone which in and of itself will not make you taller(unless you have open plates).
Unless these forces increase intramedullary pressure, which all these forces have been shown to increase intramedullary pressure(Exercise training augments regional bone and marrow blood flow during exercise), they are probably not going to make you taller. The problem is these forces do not increase intramedullary pressure enough. Muscular contraction is indirect loading and limited by muscle size and speed by which you contract the muscles. Imagine the bone is a balloon. The muscle is the pump. The air is going out and you have to pump it faster than it’s going in. Whether the balloon gets pumped(high enough intramedullary pressure) depends on the strength(size of muscle) and speed of the pumps(speed of contraction). Axial loading does not really drive fluid flow as well as lateral loading.
Maybe electrical muscular stimulation can make for above normal muscular stimulation but if the contractions are very rapid they’re unlikely to be able to be very strong.
The goal of impact loading is to bypass the limitations of muscular contraction and directly increase intramedullary pressure. The goal of lateral loading is that it is more effective than axial loading in driving flow.
Femoral venous ligation has been shown to increase bone length in (growing 8 week old) rats. Veins take blood towards the heart so they decrease intramedullary pressure. In that study Intramedullary Pressure was only increased by 50%. Imagine if the pressure was higher.
I believe that the key to growing taller involves passing an intramedullary pressure threshold and that lateral impact loading may be the key to passing that threshold.