This below study indicates that Myo-inositol can increase mandibular condylar cartilage growth but mandibular condylar cartilage can keep growing so we can’t be sure if this applies to long bones but it’s still promising. Myo-inosotol is available for purchase and it’s relatively cheap.
From WebMD “Inositol, also called myo-inositol, D-chiro-inositol, or hexaphosphate (IP6), plays a critical role in the body’s cellular growth. Though it used to be referred to as Vitamin B8, inositol is not actually a vitamin.”
Inositol is already in foods such as beans, bananas, nuts, raisins,and brown rice.
So the question is whether additional supplement is necessary and whether that additional supplementation can result in longitudinal bone growth.
Mandibular Endochondral Growth Is Specifically Augmented by Nutritional Supplementation with Myo-Inositol Even in Rabbits
“At present, functional orthodontic appliances are used for stimulating mandibular growth in pediatric cases{bite jumping appliance also has potential to work post skeletal maturity}. However, the effectiveness of functional appliances is not always stable in daily practices. A more effective, reliable, and safer therapeutic method for mandibular growth promotion would be helpful for growing mandibular retrognathism patients. As we previously discovered that nutritional supplementation of myo-inositol in growing mice specifically increases mandibular endochondral growth{maybe it could enhance growth of other cartilage} we performed preclinical animal experiments in rabbits in this study. Briefly, six-week-old male Japanese white rabbits were fed with or without myo-inositol supplementation in laboratory chow until 25 weeks old, and 3D image analysis using micro CT data and histological examinations was done. Myo- inositol had no systemic effect, such as femur length, though myo-inositol specifically augmented the mandibular growth{so we have to investigate why that is, perhaps myo-inositol could be combined with other supplements to grow taller}. Myo-inositol increased the thickness of mandibular condylar cartilage. We discovered that the nutritional supplementation of myo-inositol during the growth period specifically augmented mandibular growth without any systemic influence, even in rabbits. Our results suggest the possibility of clinical use of myo-inositol for augmentation of the mandibular growth in growing mandibular retrognathism patients in the future.”
The fact that they think there might be clinical use is promising as it again it is available in foods so it suggests that supraphysiological doses might be helpful.
“A functional appliance is reported to induce mandibular growth by augmentation of endochondral growth in mandibular condylar cartilage and remodeling of the temporomandibular joint”<-this would be amazing if we could get it to happen in other joints and could be the key to growing taller
“nutritional supplementation of myo-inositol in growing mice specifically increases mandibular endochondral growth”<-however mice may not have as diverse a diet as humans
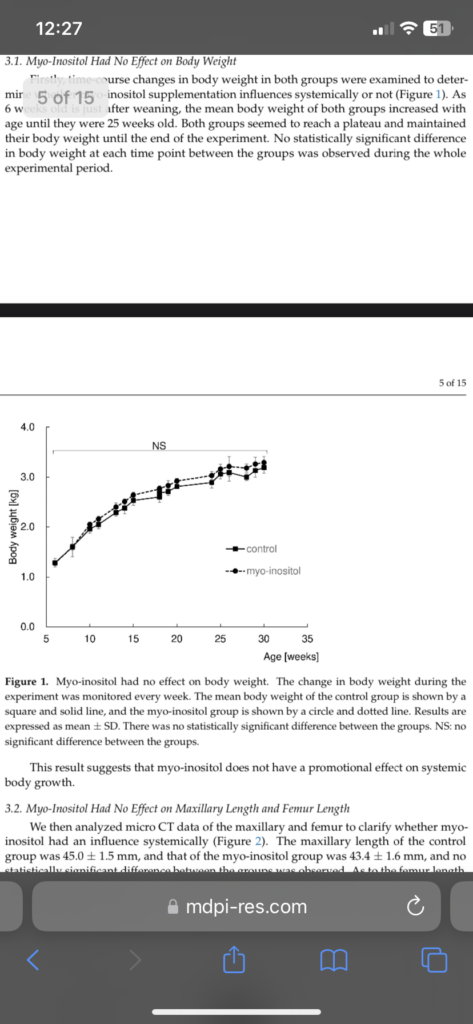
They suggest that mayo-inositol likely did not have systemic effect on growth as there was no change in body weight but if you look at the image you see a slight increase versus control.
However this sentence is not promising “
e myo-inositol group was 90.6 ± 1.1
group was 45.0 ± 1.5 mm, and that of the myo-inositol group was 43.4 ± 1.6 mm, and no mm. There was no statistically significant difference between the groups in femur length.
This result suggests that myo-inositol does not have any promotional effect on bone
statistically significant difference between the groups was observed. As to the femur length,
the control group was 91.3 ± 0.9 mm, and the myo-inositol group was 90.6 ± 1.1 mm.”
However the rabbits(Japanese white rabbits) were given the doses at 6 weeks old and sacrificed at 25 weeks old which is pretty young so it’s possible that growth was slowed but the growing period was elongated. Rabbits stop growing between 5-18months.
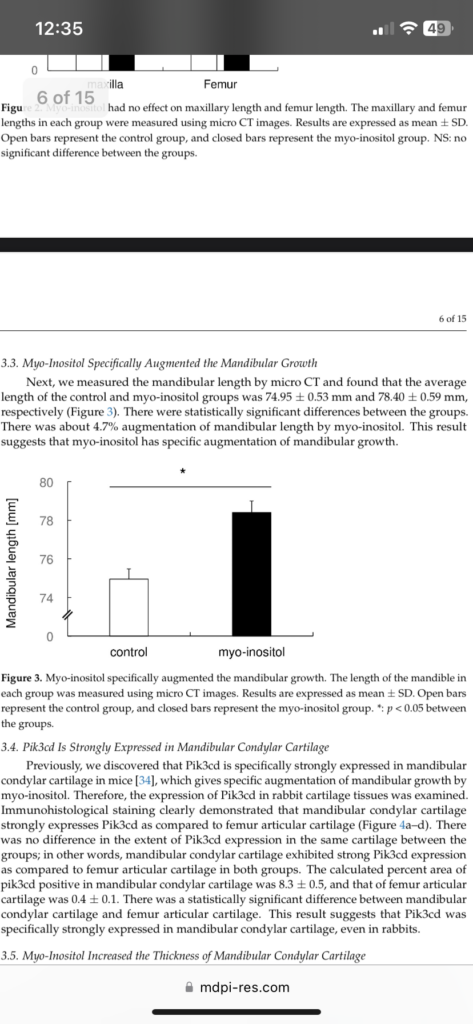
Myo inosotol significantly increased mandibular length
“discovered that Pik3cd is specifically strongly expressed in mandibular condylar cartilage”<-maybe we can increase this expression other cartilages to make them grow.
“growth augmentation of the mandible with myo-inositol requires no local injection but just simply needs to supplement the food.”
So the big takeaway here is to make sure you’re getting enough your diet but perhaps we have to find a way to upregulate Pik3cd to grow other joints.
“growth augmentation in the mandible by supplementation of myo- inositol, it was 4.7% induction in our experiments using rabbits. Our previous experiment revealed 8.4% induction in mice”
“inhibition of Pik3cd by a chemical inhibitor almost completely inhibited myo-inositol-mediated augmentation of chondrocyte proliferation in mice”
So next actions for height seekers are definitely to to see if we can increase Pik3cd in other joints to make them more like mandibular condylar cartilage.