While we have all been thinking about mechanical ways on how to possibly pull bones apart to lengthen them, I came to realize that there may be a simpler way to lengthen bones, using certain basic physics principles that we have not thought about.
What I am going to propose is that maybe it is possible to use magnetic fields to create forces which can cause the bone sections to pull apart from each other.
I am reminded of the idea of applying a capacitative electrical field through two metal electrodes attached to lateral sides of the growth plate region in teens and children with open growth plates to accelerate longitudinal growth. It was proposed by Dr. Carl Brighton in the landmark patent and study below…
Other studies were written by researchers who were doing very similar research
I still need to refer to the paper “Electrical Stimulation in Tissue Regeneration” to fully understand just how human tissue and cells would react from applied electrical signals.
The point is to show that beyond using a contant capacitive electric field to stimulate growth plates to increase the growth process faster, it might be possible to use the other half of the Electromagnetic Field & Waves phenomena for height increase purposes.
If we remember from elementary school science, there is the North and South Poles of any magnet and they attract each other. If we had two North or two South Poles, they would repel each other.
I am proposing that it might be possible to create two poles that are the same on opposite sides and induce them to pull away from each other and having the metallic rods or rings held to the human bone.
With a AC electrical signal, we can induce a magnetic field that increases in strength and then decreases like a intermittent way to push at the bones.
Let’s look over some introductory university level electromagnetic theory. There is no mathematics, just some conceptual electromagnetic reasoning.
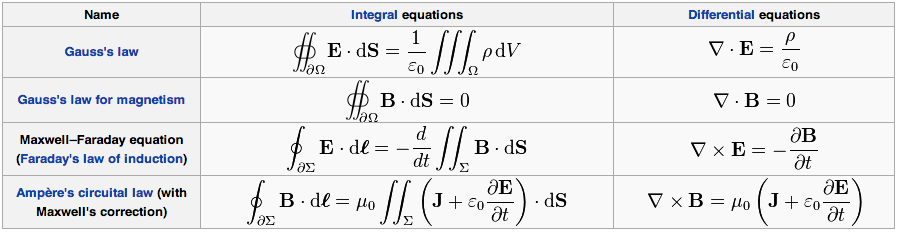
First, I have clipped the chart for the Differential and Integral form of Maxwell’s Equations from the Wikipedia article on Maxwell’s Equations
Side Note: If any person can manage to prove the existence of magnetic monopoles, they would validate many of the ideas of string theory and definitely receive a Nobel Prize in Physics for this achievement. I have taken an advanced level undergraduate electrodynamics course using the standard Introduction to Electrodynamics, 3rd Ed. by Griffiths so I should still remember a little bit of the course still.
In general, when one sees the symbol for an integral, where it is a double integral, triple integral, closed path integral, line integral, surface integral, the basic idea is that you are to sum everything that is specified together. The term integration basically means to add all of the possible alternative ways together.
This is my personal level of conceptual understanding of the 4 main laws.
Guass’s Law – When you add together all of the Electrical Fields, E over a closed surface, you would get a charge density divided by a universal constant. For practical purposes just forget the constant and realize that the whole point is to calculate a quantity of charge and Electrical Field in a 3-D space.
Guass’s Law of Magnetism – The Integral form suggest that if you add together all of the Magnetic Field, B in a closed surface, the net result is 0. The reason that the net magnetic field is 0 is because of that fact that magnetic fields are derived from a dipole system. Everything that has a origin will also end up back in the same origin at the end of the path.
Closed Surface – The concept of a closed surface is important. The idea is to create an imaginary boundary condition, like a infinitely thin spherical shell which will encapsulate the system one would try to calculate the net charge is in the region that is defined by the boundary conditions.
Faraday’s Law Of Induction – This is the first of the two other laws of the four which is slightly more complicated so I wanted to break the conceptual understanding down into looking at both the Integral Form and the Differential Form
- Integral Form – When you add together all of the Electrical Fields, E in a closed path, using a line integration you would find it equal to the change in time of the sum of the Magnetic Fields, B added together in a specific surface that is also going in the opposite direction
- Differential Form – We can create an electrical field by changing the magnetic field
Ampere’s Circuital Law w/ Maxwell’s Correction
- Integral Form – The combined total of all the Magnetic Field in a closed path loop is equal to the change in the combined Electrical Field added with a hidden electric field over a surface, both multipled by a certain special constant which is over a given specific surface
- Differential Form – An Electric Field and a change in Electric Field will both lead to the creation of a magnetic field
Implications For Height Increase Applications
If we look at the last two equations of Maxwell’s E&M , and remember back to the way that induced magnetic fields from electrical work and which direction they go in, it seems reasonable to think that we can induce a magnetic force that would push two electrical hard wires farther apart from each other. If the wires are also somehow held in place against bone tissue, then they can theoretically over time using magnetic force pull bone tissue apart.
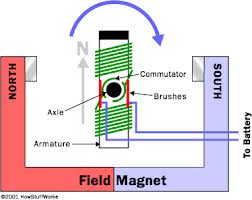 Let’s look back at how the common electric motor works, even those that one finds in plastic toy cars.
Let’s look back at how the common electric motor works, even those that one finds in plastic toy cars.
The power source is a battery, which is DC electrical source. The electrons inside the copper wires go down the wires which is connected to the battery which is how current is created. The electrons that create current will create charges, which results in a electrical field. From Faraday’s Law of Induction, the wire does form a closed path since the wire is connected in a way for a closed circuit to the battery. This causes both a magnetic force and a change in magnetic force. Since there is already magnetics put in the system, when there is a magnetic field, S or N, the force between the created magnetic force which is changing and the magnetics already in place will cause the magnetics to either attract or repel each other.
To create the alternation that is needed to change, what are known as brushes to close and open the wires forming either closed or open paths are needed in the system.
 The point is that it is reasonable to create a two non-magnetic metal ring system which will have electrical current run through them, which will induce the metal into a magnet, and they will develop the repulsive force and pull themselves away from each other.
The point is that it is reasonable to create a two non-magnetic metal ring system which will have electrical current run through them, which will induce the metal into a magnet, and they will develop the repulsive force and pull themselves away from each other.
At this point, the theory makes sense but I am not sure how to design the actual device. It is totally possible that this proposed idea is not viable since people may reject the idea of having metal rings embedded deep onto the surface of the bones.
Just refer to the picture on the right for reference. Of course it would be difficult to embed the metal in the first place into the bone if they are already magnets. The other problem is that the magnetic force of the small magnet to the right are too weak so that is why we need to have ferromagnetic metals which when they have a current passed through them, they turn magnetic. Not only that, the more current that can be passed through, the stronger the magnetic field can become and the harder the metals will try to pull apart from each other, thus distracting the bones that they are embedded or attached to.
There is also a second part. It is critical if we think that an induce magnetic field from a battery current would even work.
It is to make the area of bone that we are trying to distract weaker. Like I said multiple times before, the bones are just too hard and strong and brittle to pull apart using normal devices. I calculated in the post “The Values For The Magnitudes For The Forces And Loads Needed To Increase Epiphyseal Cartilages Thickness And Human Femur Bone Without Fracture (Important)” that it would require about 25,000 – 30,000 lb of tensile loading force to pull the adult human femur apart elongating it, if not outright snapping it in half the moment the critical threshold, which is known as the Ultimate Yielding Strength is reached. Certain studies like “DIFFERENCES IN THE TENSILE STRENGTH OF BONE OF DIFFERENT HISTOLOGICAL TYPES“ agree that the calculated value is about right.
This means that the bones need to get weaker, at least in terms of getting the calcium hydroapatites removed, which has alway been the primary element that gives bones their hard, brittle nature. In a recent post I discovered that one can actually turn bone tissue into rubber using vinegar which is just ascetic acid.
So there is two parts to a device, one where two rings are embedded on the bones of the individual which can’t be moved and an induced current will cause the magnets to start to push themselves away.
In the middle, between the two rings, a solution of ascetic acid or vinegar is injected using small plastic needle syringes into the cortical bone layer to start to remove the calcium crystals.
The bones in just one band or layer grow weaker as the collagen is left and the bone is distracted.