
Limb lengthening surgery is only for the legs and people state that without torso lengthening people will be unproportionate(unless they already have long torso to height). So any method to increase torso length via surgery could potential be of interest to those people. Also, it could be possible to replicate a surgical method with some kind of mechanical loading or mechanical stimulation. So that makes it of interest to. But we’d have to see how exactly the mechanism by which the height increase works.
Lumbar vertebral canal stenosis due to marked bone overgrowth after routine hemilaminectomy in a dog
Stenosis is narrowing of the spinal canal which would be bad but possibly we could find ways around that. A hemilaminectomy is a surgical procedure that aims to enlarge the space in the spinal canal to reduce nerve compression or pressure. Based on how effective we believe this method could be we’d have to really understand how a hemilaminectomy works.
“Bone overgrowth after decompressive surgery for lumbar stenosis”
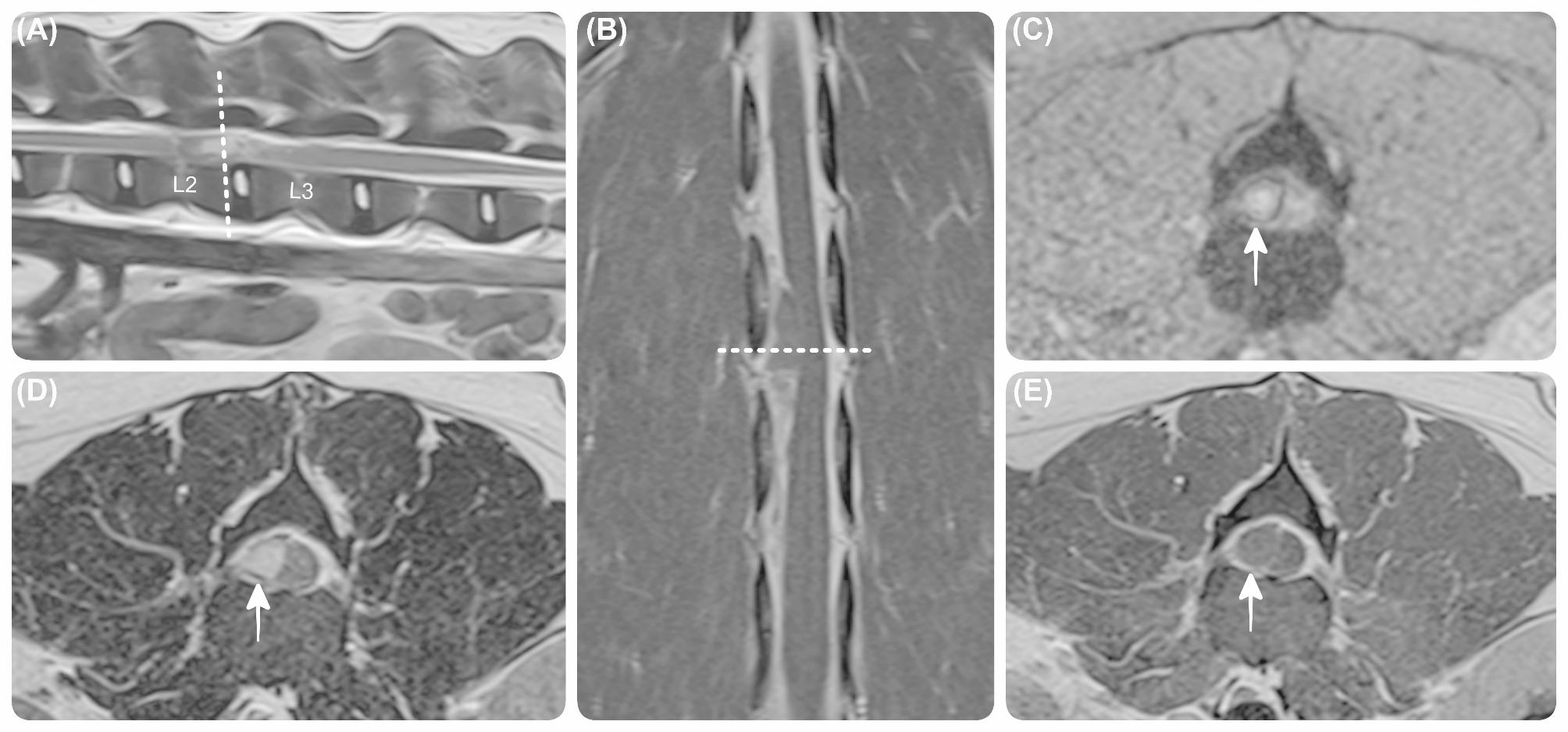
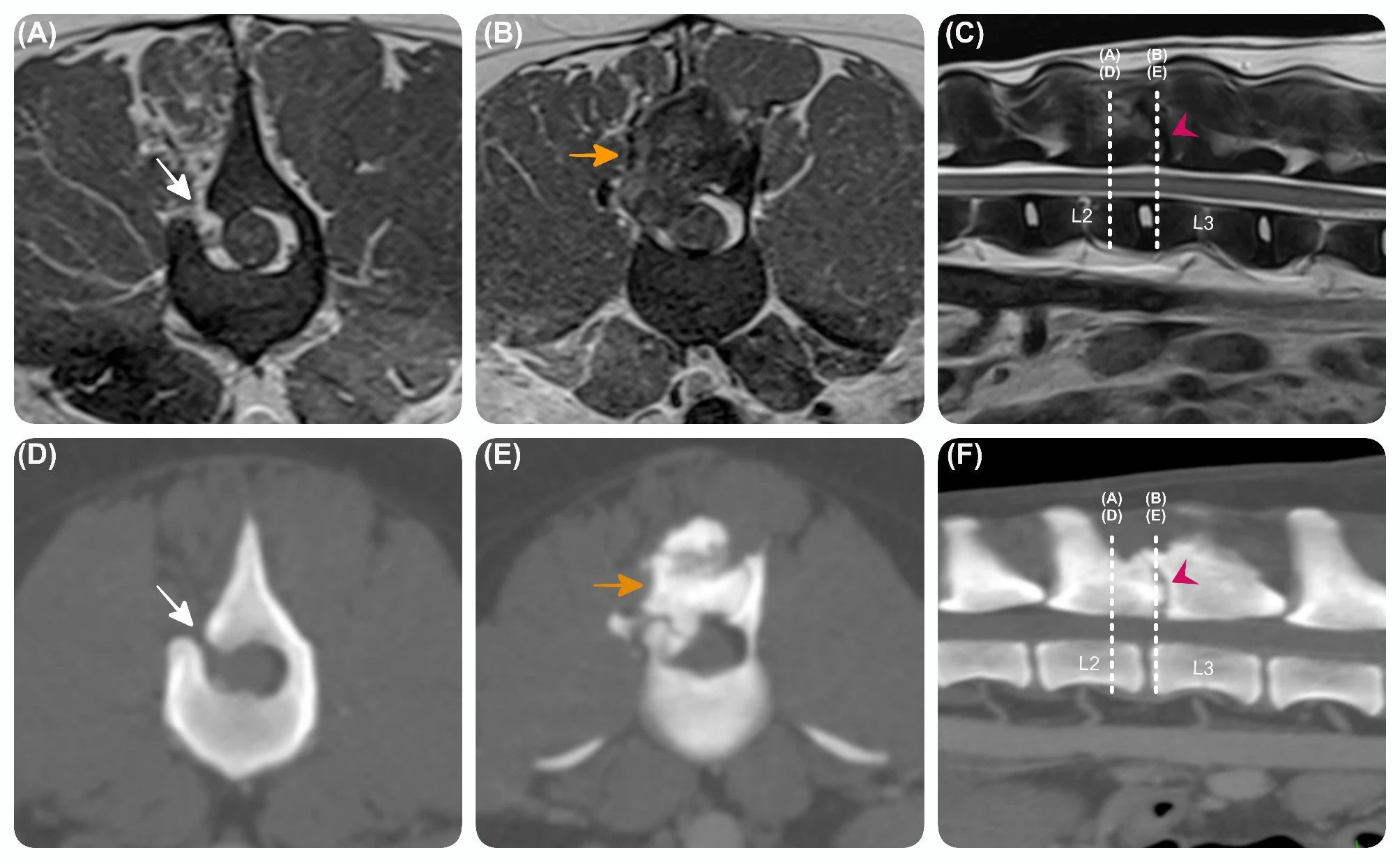
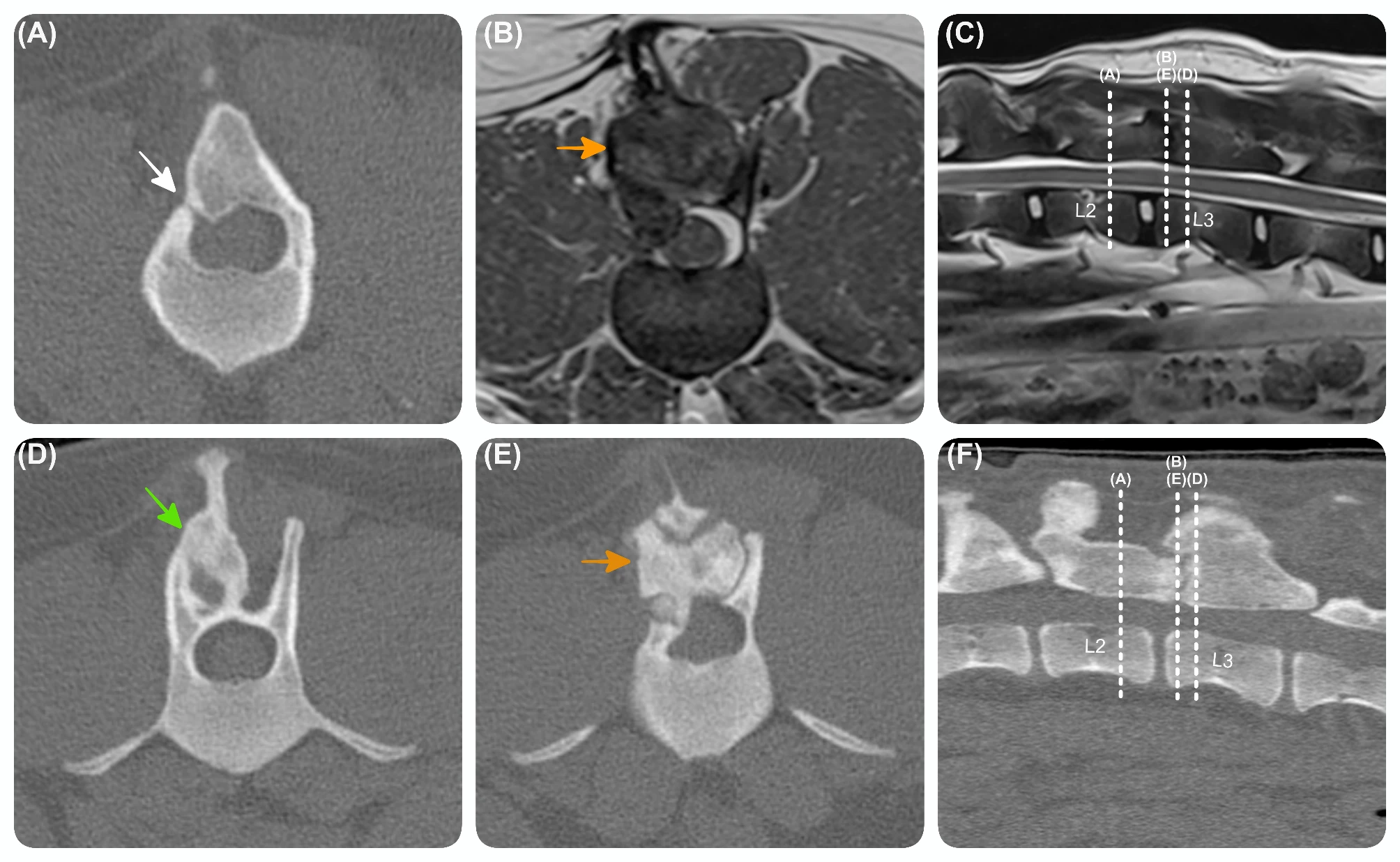
“A 13-month-old entire female dog{this is a pretty young dog}, a crossbreed between a Springer Spaniel and a Border Collie, weighing 24 kg, was referred with a 5-day history of progressive spastic paraplegia, indicative of a T3-L3 myelopathy. Magnetic resonance (MR) imaging revealed a right-sided L2-L3 compressive extradural lesion, compatible with epidural haemorrhage, which was confirmed by histopathology. The lesion was approached via right-sided L2-L3 hemilaminectomy and was successfully removed. One-year postoperatively the dog re-presented with pelvic limb ataxia. MR and computed tomography (CT) images demonstrated excessive vertebral bone formation affecting the right articular processes, ventral aspect of the spinous process of L2-L3, and contiguous vertebral laminae, causing spinal cord compression. Revision surgery was performed, and histopathology revealed normal or reactive osseous tissue with a possible chondroid metaplasia and endochondral ossification, failing to identify a definitive reason for the bone overgrowth. Nine-month postoperatively, imaging studies showed a similar vertebral overgrowth, resulting in minimal spinal cord compression. The patient remained stable with mild proprioceptive ataxia up until the last follow-up 18 months post-revision surgery.”<-unexplained bone overgrowth is good because it could indicate that there’s a possible height growth mechanism that we’re not aware of yet.
“Bone healing depends on the initial inflammatory phase, both local and systemic, in response to the injury. The repair phase is characterised by the formation of a soft callus, consisting of fibroblasts, chondrocytes, and osteoprogenitor cells. The new extracellular matrix produced by these cells serve as a temporary scaffold for bone formation. This phase involves the recruitment and differentiation of mesenchymal stromal cells (MSCs), which have the potential to differentiate into osteoblasts, promoting bone regeneration and bridging the fracture site. The remodelling phase is the final stage of bone healing, where the newly formed bone undergoes structural and functional modifications, restoring the bone’s normal architecture”
“In human medicine, bone overgrowth is an uncommon but important cause of relapse of neurological signs after decompressive surgery in elderly patients undergoing treatment for lumbar spinal stenosis, most performed at the L4-L5 level”
“factors such as segmental instability, micromotion, and abnormalities in mechano-signalling have been hypothesised to contribute to the excessive bone regrowth”<-we could potentially mimic things like segmental instability
IF you look at the next set of slides however
“[bone overgrowh] is commonly observed at the L4-L5 level, known to be the most mobile intervertebral level in humans”<-this is interesting because it potentially means that movement can influence growth but it could also indicate that cartilage degeneration is what initiates growth.
“Histopathological evaluation showed the presence of normal or reactive osseous tissue, rather than new bone and immature woven bone. This finding may be similar to heterotopic ossification reported in humans following trauma or injury. The presence of chondrocytes in some fragments could indicate a possible chondroid metaplasia and endochondral ossification, which are necessary for bone regrowth“<-the dogs were young so initiation of endochondral ossification is not terribly exciting but similar processes seem to occur in the elderly as mentioned in the study which makes it more exciting.
Overall this paper may hold something for the future but it is not really anything to write home about now.