
While I was doing research on how the alignement of a double growth plate would lead to potential unlimited lengthening of the long bones, I took a deeper look at how the ossification centers and realized something which I was surprised I had missed before.
In one of the most important posts written for the website where I had analyzed how the antlers in some deer fall off and regrow in length each and every year, I had noted that to be able to get the type of lengthening you need to have a tip area which has mesenchyme, and that it must be covered by a type of tissue that is either perichondrium, or has the elastic and impermeable nature of perichondrium.
The posts were
- The Connection Between Regenerating Deer Antlers and The PTHrP, PTH And IHH pathway for Cartilage Regulation, PTHrP Seems To Be The Answer (Big Breakthrough!)
- Increase Height And Grow Taller From Deer Antler Regeneration Principles
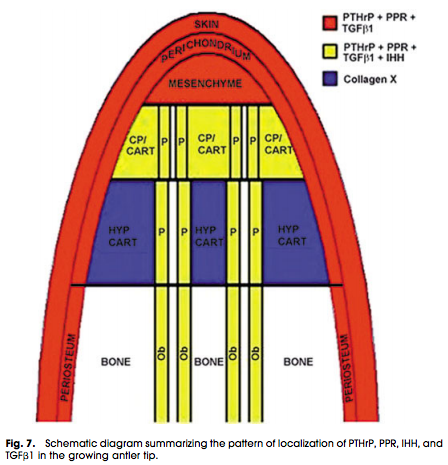 See the diagram on how tissue would have to align for any type of tissue expansion to happen.
See the diagram on how tissue would have to align for any type of tissue expansion to happen.
You see that the bone has to be at the bottom, while at the edge or tip, it has to have the progenitor cells/mesenchyme ready to differentiate into the chondrogenic lineage which is will what be the tissue that can really expand the structure volumetrically.
Now, Let’s look at the tip or ends of a long bone to see the difference. The long bones are growing longer or longitudinally because the growth plates are pushing the bony secondary ossification center outwards away from the primary ossification layer.
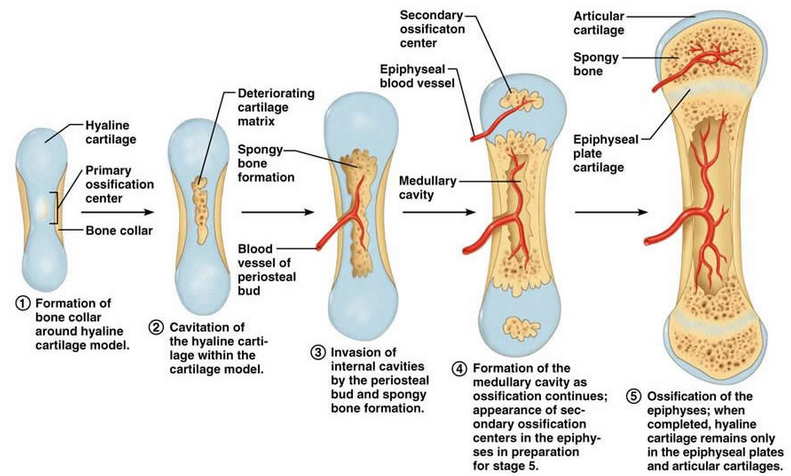
The ends or tip of the bones, which are known as the epiphysis have a core of ossified cartilage (aka bone tissue) and that grows out until it envelops all of the tissue of the structure at the knobby ends of the long bone except for the articular cartilage.
However the thing that I noticed in this picture which may not be shown in other anatomical diagrams of bone tissue is that there are blood vessel that are going into the epiphysis and the diaphysis. I had forgotten about a very important point which I had researched months ago as well as also forget one of the most basic points of the cartilage-bone tissue relationship.
The first thing I forgot was that there was a study that showed that if you take an awl, and put the awl in a hole that was made from a drilling into the diaphysis of the long bone, and then turn the awl around, basically cutting the blood vessels thus restricting the blood vessels and nutrients from reaching the various regions of the long bone, you notice that the longitudinal growth of the long bone seem to increase slightly.
The 2nd thing that I forgot was that for cartilage to ever turn into bone, it has to go through a process where it’s protective covering, the perichondrium has to start to fail in its strength, the cartilage get invaded by blood vessels that gets inside, and over time, the vascularization leads to the introduction of calcium minerals, leading to then mineralization and calcification, and thus ossification.
Proposed Method For Height Increase
We can get the long bones to ‘grow’ or lengthen by making sure that the ends keep on pushing away from it. As long as the end of a bone structure is filled with material that is not bone, or at least not completely made form bone tissue, just as the case with the tip of the antlers in deer structure. The bone was the tissue at the base but at the tip was only mesenchyme that would turn into cartilage. Somehow the mesenchyme never turned into bones themselves until the mesenchyme was completely used up.
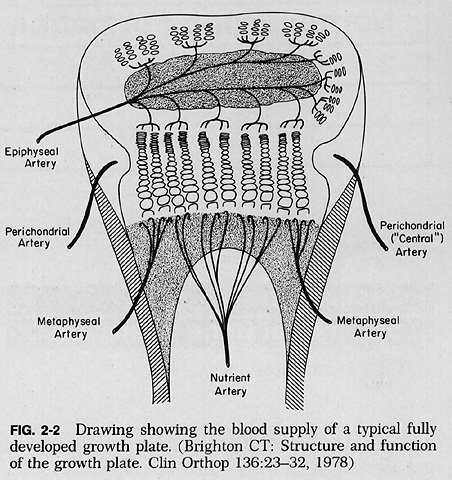 We see from many anatomical diagrams that there is at least one major blood vessel going through the epiphysis of the long bones to supply it with the proteins and nutrients to continue to make organic living cells like the mesenchymal stem cells that are in the epiphysis. However that blood vessel is also the main cause of the epiphysis/ ends of the bones turning into bones through ossification in the first place. There is one famous study that shows that if you disrupt the blood vessels going into the metaphysis (or the diaphysis) of the long bone, the longitudinal growth of the overall bone is increased. This shows the possibility that if you disrupt the blood vessels that are doing the vascularization of one of the sides of the growth plate, the bone is supposed to get longer.
We see from many anatomical diagrams that there is at least one major blood vessel going through the epiphysis of the long bones to supply it with the proteins and nutrients to continue to make organic living cells like the mesenchymal stem cells that are in the epiphysis. However that blood vessel is also the main cause of the epiphysis/ ends of the bones turning into bones through ossification in the first place. There is one famous study that shows that if you disrupt the blood vessels going into the metaphysis (or the diaphysis) of the long bone, the longitudinal growth of the overall bone is increased. This shows the possibility that if you disrupt the blood vessels that are doing the vascularization of one of the sides of the growth plate, the bone is supposed to get longer.
The proposed idea is to drill a small hole into the epiphysis and disrupt the blood vessels going into the epiphysis, to keep the tissue in the epiphysis in a relatively large percentage of cartilage tissue. My proposal is that as long as the ends of the long bones are not completely infiltrated by blood vessels, they will stay in a state more like a the tip of the antlers of deer, which has the possibility of turning into chondrocytes and this means that the lengthening of the ends of long bones becomes a possibility.
So there are two parts.
1. Drill a hole into the epiphysis and disrupt the vascularization of the ends of the long bones. This would help keep the entire region from turning into bone tissue.
2. Inject through syringe around 50 ng of BMP-7/OP-1 per gram of tissue into the hole. I have stated recently that out of all the BMPs, the BMP-7 seem to have the most chondrogenic benefits. This would help in turning any mesenchyme/ progenitor cells that did not get destroyed to convert into chondrocytes and possibly then cartilage.
The result is the epiphysis/ends of the long bones becoming softer, more elastic, and more like the tips of deer antlers which can push out and lengthen the ends of the long bones.
The post that really got the core idea started is “Studying Changes In The Growth Plate By Restricting The Blood Vessel Supply, Ischaemia” where I referenced a very old study done by a surgeon named Albert B. Ferguson named “SURGICAL STIMULATION OF BONE GROWTH BY A NEW PROCEDURE – PRELIMINARY REPORT“. Ferguson was also the man who showed to me one of the most crucial ideas on how to possibly increase height using a very practical idea which can be easily done at the comfort of one’s home, which I had coined the Chisel and Hammer method, which I would show in the YouTube Video “Chisel and Hammer Method Explained“. The basic idea behind the Chisel and Hammer Method is to break apart the periosteum layer so that the growth plate tissue would be less restrictive in their ability to expand.

