
An increase in articular cartilage thickness will result in a slight increase in height. There have been studies that show that mechanical loading can increase this cartilage thickness in some bones. Whether the articular cartilage can increase in thickness could be affected by whether it is bound by the periosteum or not. Some bones such as the fingers can grow longer and are not bound by periosteum.
Longitudinal change in femorotibial cartilage thickness and subchondral bone plate area in male and female adolescent vs. mature athletes.
“The objective of this study was to explore longitudinal change in femorotibial cartilage thickness and tAB[Subchondral bone area] in adolescent athletes, and to compare these data with those of mature former athletes. Twenty young (baseline age 16.0±0.6 years) and 20 mature (46.3±4.7 years) volleyball athletes were studied (10 men and 10 women in each group). Magnetic resonance images were acquired at baseline and at year 2-follow-up, and longitudinal changes in cartilage thickness and tAB were determined quantitatively after segmentation. The yearly increase in total femorotibial cartilage thickness was 0.8% in young men and 1.4% in young women; the gain in tAB was 0.4% and 0.7%, respectively. The cartilage thickness increase was greatest in the medial femur, and was not significantly associated with the variability in tAB growth. Mature athletes showed smaller gains in tAB, and lost >1% of femorotibial cartilage per annum[year], with the greatest loss observed in the lateral tibia. In conclusion, we find an increase in cartilage thickness (and some in tAB) in young athletes toward the end of adolescence. Mature (former) athletes displayed high rates of (lateral) femorotibial cartilage loss, potentially due to a high prevalence of knee injuries.”
“X-rays are not capable of delineating soft tissues and cartilage”
“articular cartilage volume growth in the tibia (but not in the patella) correlated significantly with change in body height, and that – in terms of cartilage volume gain – overweight children did not differ significantly from those with normal weight. Finally, tibial cartilage volume gain was greater in those who reported an average intensity of sport above the median”
“a longitudinal gain in cartilage volume and thickness was observed post-injury[ACL rupture] and was interpreted as a potential sign of (pathological) cartilage swelling”
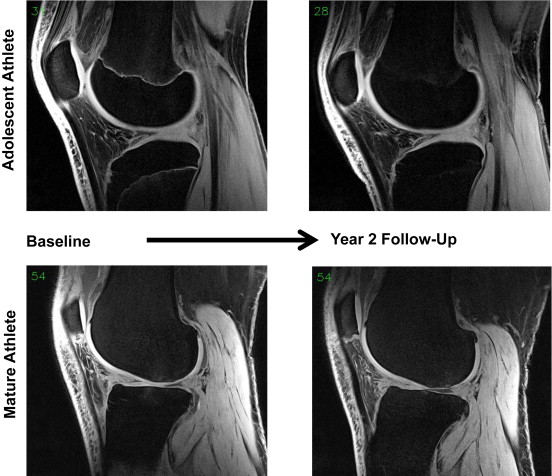 Comparison of adolescent and mature volleyball player knee by MRI.
Comparison of adolescent and mature volleyball player knee by MRI.
“Adolescent men and women tended to have smaller cartilage thickness than mature participants in the medial femorotibial compartment, but greater thickness than mature adults in the lateral compartmen”
“Lateral compartment cartilage was thicker than medial compartment cartilage across all sex and age strata. Medially, the femoral cartilage was thicker compared to the tibial cartilage, while laterally, the tibial cartilage thickness was thicker compared to the medial cartilage; again, this was consistent across all sex and age strata”
“the study lacks a reference group of less physically active adults without knee injuries”
Perichondrium is key to regenerative potential of articular cartilage and unfortunately it does not cover the joint region.