
I think this idea that I recently discovered called the Somatomedin Hypothesis is going to challenge some of the basic ideas we have been using since the start to explain how the GH and IGF-1 feedback loop really works to control endochondral ossification.
I refer to the 3 studies below as reference to make the point.
- Study #1: The somatomedin hypothesis 2007: 50 years later.
- Study #2: The somatomedin hypothesis: 2001
- Study #3: The somatomedin hypothesis revisited in a transgenic model
Background
GH, or the natural type of human growth hormone found in the human brain’s pituitary gland anterior region was one of the first compounds ever to be discovered and synthesized. Other names for GH, growth hormone are somatropin and somatotropin. Synthetic types of growth hormones have been made for many decades now and the different variations include Syntropin, Nutropin, Humatropin, etc.
After doctors and researchers reached the conclusion that GH is the thing that controls human growth, specifically vertical growth in terms of growing taller, the proposed idea was that there is supposed to be a proxy, an intermediate compound between the actual GH that is made in the pituitary gland and it final target areas, which are the receptors on the chondrocytes in the growth plate.
The old idea proposed was that this intermediate compound is known as somatomedin. Later it seems that Somatomedin was replaced with the now more commonly well known name, IGF-1 after the compound was understood much better through further research.
Somatomedin C = IGF-1
The idea back then was that somatomedin was produced by the liver in response to the release of GH into the system. Then the somatomedin would be the actual compound that affects the receptors on the chondrocytes in the growth plate by going through the circulatory system.
The reason why it was believed that GH was not the compound that affects the chondrocytes in the growth plate direclty, but required an intermediate was because while injecting the extracted and purified GH into a lab animal did lead to the growth plate getting thicker and expand more, when the growth plate cartilage was extracted out an animal and put in a culture and then had the GH added, there was no increase in thickness. So the scientists believed that there had to be a 2nd compound that the GH caused to initiate. So in vivo, GH worked. In vitro GH didn’t work.
This was the entire premise of the original somatomedin hypothesis.
The picture below as taken from the study “The Somatomedin Hypothesis 2007: 50 Years Later”
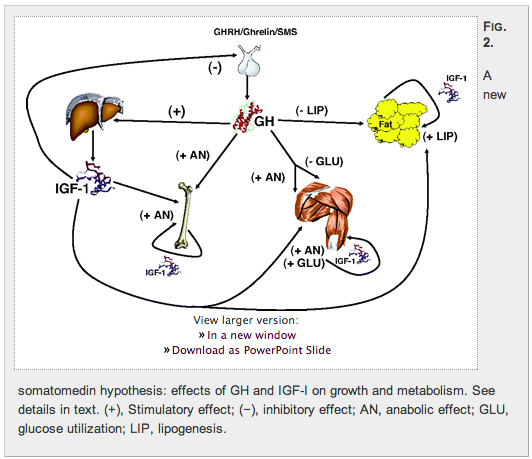
Conclusion
The researchers notes that after 50 years, the original somatomedin hypothesis must be changed due to the following 4 reasons…
1. Investigators have shown that, under the proper conditions, GH does indeed exert a direct action on precursor incorporation in the in vitro cartilage system.
2. There is a substantial body of evidence that GH acts directly (and independently of IGF-I) on the growth of bone.
3. Although the liver is the main source of IGF-I in the circulation, IGFs are produced in virtually every tissue of the organism.
4. GH receptors have been shown to be present in virtually every tissue.
They tried to find someone who could come up with a theory to explain for all of the noticed new discoveries for the function of GH and not one theory could explain everything that was going on with GH. So the researcher made their own model or theory to explain how IGF-1 really is connected to GH in function.
This is what they proposed…
We propose that the IGFs, rather than effectors of GH action, are augmentative hormones that amplify the anabolic actions of GH while countering its potentially deleterious effects. Because the IGFs are counteractive for some but not all the effects of GH, their insulin-like effects may act to negate GH-stimulated gluconeogenesis and enhanced lipolysis.
Analysis
This means that the IGF-1 are not the type of hormone that only increase when GH increases and only helps out the function of GH. There are some functions where the IGF-1 negates the effects of GH, and that means that our original idea that IGF-1 is the main type of hormone/protein that can get to the growth plate cartilage is wrong. GH can directly interact with the growth plates.
The exact way that IGF-1 contributes to the function and effects of GH is by helping GH in anabolic activities and somatic growth. When it counteracts the effects of GH, it is to prevent the GH from causing diseases like hyperglycemia and loss of lipid stores. So the lipid and carbohydrate metabolism effects of the IGF-1 and GH in action concurrently are exactly the opposite.
The main thing is to show that the old somatomedin hypothesis is not completely right and needs to be modified. The four reasons are…
- GH does indeed exert a direct action on precursor incorporation in the in vitro cartilage system.
- There is a substantial body of evidence that GH acts directly (and independently of IGF-I) on the growth of bone.
- Although the liver is the main source of IGF-I in the circulation, IGFs are produced in virtually every tissue of the organism.
- GH receptors have been shown to be present in virtually every tissue
The GH themselves have a much more direct affect on chondrocytes that previously expected.