Note: I seem to remember that I might have already done a post on this diagram I have pasted below in this post before months before. Given the large number of posts I have written, my memory is not clear on which post that was. So I guess it is okay if I decided to redo an old post all over again, just so that it can be a review for me on the concepts and results.
This is one of those chart, tables, or diagrams which show that the research we have been doing is on the right track ,or at least that we are finally being good enough in our readings to know that what we have been hypothesizing is validated by other scientific works.
From the PubMed study & article “Concepts in Gene Therapy for Cartilage Repair“…
Analysis & Interpretation
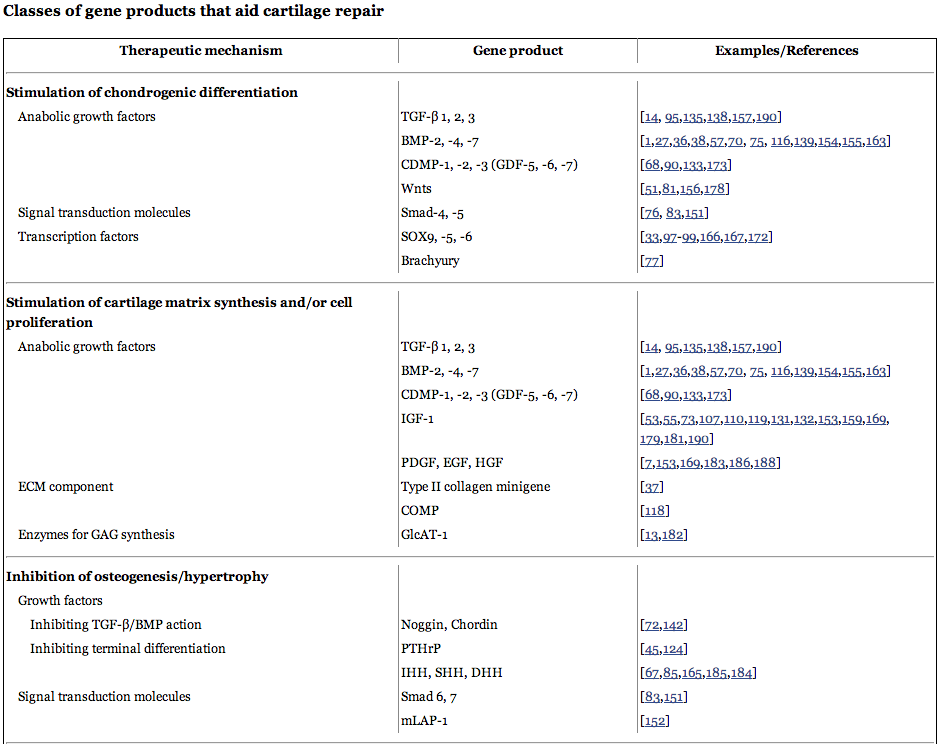
I note that the growth factors in the chart are only for chondrogenesis and cartilage generation. This is good because so often when we are talking about the skeletal structure, we only are focused on the growth factors which will be best for osteogenesis, since most studies on bones and cartilage are for chronic, old age issues like osteoperosis and rheumatic arthritis, which are caused by bone mineral density decreases and cartilage degeneration. Nobody has done any research to see the research of cartilage generation from the lens towards height increase.
The chart below is rather big and complicated but the main point is that almost everything listed below has anabolic aka growth potential to make cartilage grow from at least progenitor mesenchyme cells if they are there.
So let’s go down the list.
We have seen the TGF-Betas before, type 1 and 2. Type 3 I am not familiar with.
We have the BMPs, 2, 4, and 7 which we have done extensive research on and they seem to be better at getting multipotent stem cells to differentiate into the chondrogenic lineage than the ostegenic lineage.
The CDMP stands for Cartilage Derived Morphogenic Protein. It seems that they go by a more familiar names, the Growth Differentiation Factors, and I have stated in at least two previous posts, (“Is Growth Differentiator Factor 5 GDF5 Gene The Most Influential Gene Towards Height?” and A New Proposed Theory To Increase Height And Grow Taller Using GDF-5 (Breakthrough!)) that GDF-5 has potential to be huge in our goals to become taller. As for GDF-6 and GDF-7, I did a post about the whole group of GDFs many month ago entitled “A Detailed Study And Analysis On Growth Differentiation Factors GDFs Which Influence Growth And Height” and I seem to remember that only 2 of the many GDFs had potential to be used as a growth factor for chondrogenesis. However I will look into the reference studies listed.
We have Smad which is both the gene that creates the protein, and the protein, but I have not done any research on it yet.
The Sox9 gene was shown to be critical in the post “Why Does The Epiphyseal Cartilage Disappear But The Articular Cartilage Remain? (Breakthrough!)” which shows that for Chondromodulin Type I to work and the area of the articular cartilage to not get vascularized, we need the Sox9 gene to be turned on.
The IGF-1 is very well known by researchers to have chondrogenic effects since it seems to be able to directly effect the receptors on the surface of chondrocytes.
Everything else, like the Brachyury, mLAP1, PDGF, EGF, HGF, Comp, etc. I have never even heard of.
What might be better for me to relearn the growth factors and proteins that help in cartilage regeneration is to look at the sections the chart is broken into,
Stimulation of Chondrogenic Differentiation
- Anabolic Growth Factors
- Signal Transduction Molecules
- Transcription Factors
Stimulation of Cartilage Matrix Synthesis and/or Cell Proliferation
- Anabolic growth factors
- ECM Component
- Enzymes for GAG synthesis
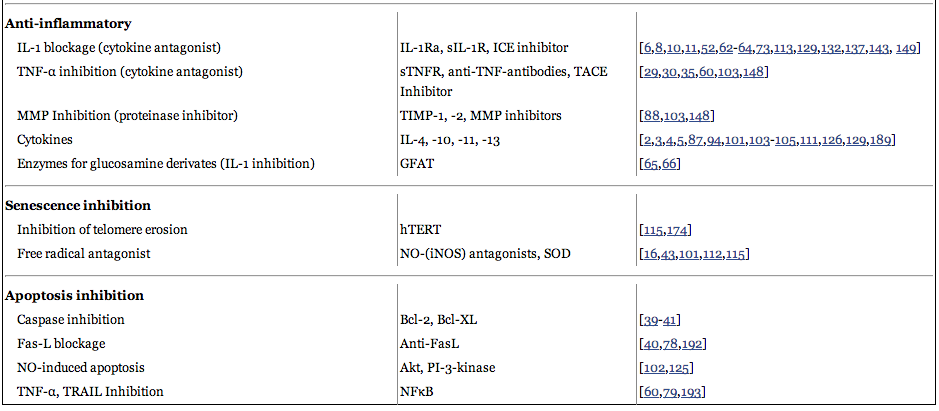
Inhibition of Osteogenesis & Hypertrophy
- Growth factors – 1. Inhibiting TGF-Beta & BMP action, 2. Inhibiting terminal differentiation
- Signal Transduction Molecules
Anti-Inflammatory
- IL-1 blockage (cytokine antagonist)
- TNF-2 inhibition (Cytokine antagonist)
- MMP inhibitory (Proteinase inhibitor)
- cytokines
- Enzymes for glucosamine derivatives (IL-1 inhibition)
Senescence Inhibition
- Inhibition of telomere erosion
- Free radical antagonist
Apoptosis Inhibition
- Caspase inhibition
- Fas-L blockage
- NO – induced apoptosis
- TNF-alpha, TRAIL inhibition
From a process point of view, we can see that multiple studies have been done to show that you can try to manipulate each stage of the cartilage or chondrocyte’s life. You can trying to inhibit apoptosis, inhibit senescence, decrease inflammation, inhibit hypertrophy and differentiation into bone cells. The more anabolic strategy is to stimulate cartilage cell division and create more of the extracellular cartilage matrix.
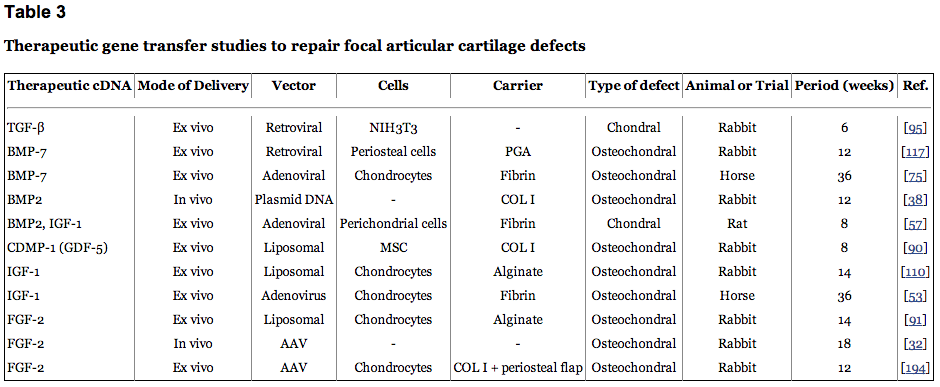
If we were just to look at the side of trying to make more cartilage and chondrocytes, we could just use Table 3, and use the BMP-2,7, the TGF-Beta, GDF-5, and IGF-1 to stimulate more cartilage growth. However it is clear from the first table that we must somehow also get the other half of the process working too so that we can prevent the cells from aging or dying too quickly, as wells keeping them from going the bone cell direction in transformations.
It seems that there are at least a dozen ways that the cartilage cells get evolved to a point which makes them none functioning. Many of the proteins and cytokines I have seen before but with little research. This table is sort of an introductory way for the researchers to see which types of PubMed studies they should be look for to understand the types of molecular mechanism which control the chondrocyte.
Implications For Height Increase
The two tables below shows us that beyond just stimulation of chondrogeniic differentiation and cartilage matrix synthesis, and cell proliferation, we would have to also consider the other side, which is how to keep them from aging and dying so we have more time to manipulate the cartilage tissue to expand and multiple in the direction which we want to lengthen long bones.