It is well circulated throughout the height increase community that tennis can induce longitudinal bone growth of the hand. The below paper discusses this phenomenon.
“This contribution addresses the following questions: Does unilateral sports-specific strain affect the skeletal system of the athlete? Specifically, can any differences be found in longitudinal growth of the bones of the forearm and hand in professional tennis players between the stroke arm and the contralateral arm? An investigation was conducted involving 20 high-ranking professional tennis players (12 male and eight female players) between 13 and 26 years of age{we’d want older players to confirm that longitudinal bone growth can be increased as adults} as well as 12 controls of the same age range. The radiologic examinations of the bones of the forearm and hand yielded an increase in density of bone substance and bone diameter as well as length in the stroke arm as compared with the contralateral arm. Whereas the first results confirm previous findings, the stimulation of longitudinal growth has never been reported. This change in bone structure and size can be attributed to two factors: mechanical stimulation and hyperemia of the constantly strained extremity{hyperemia is enhanced blood flow}. It may thus be regarded as a biopositive adaptation process”
Note that tennis involves torsion of the arm/hands, vibration when the racket hits the ball, and alterations of the bone against gravity(inversion/eversion). All of these forces are likely stimulatory of longitudinal bone growth even past skeletal maturity.
“He found an increase of bone thickness, bigger bone ledges at the insertion of muscles and tendons, and a concentration of bone structure.”<-Is there any way we can mimic the stimulatory pulling and other forces of muscles and tendons?
“an increased vascularization results in an increase in longitudinal growth provided
it takes place during the phase of general growth. Reactive hyperemia is a well-known consequence of bone fractures.”
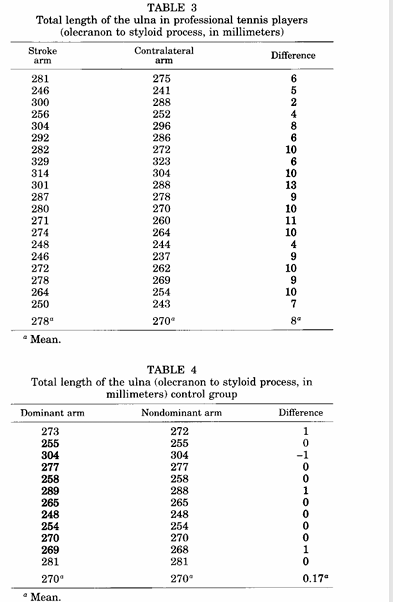
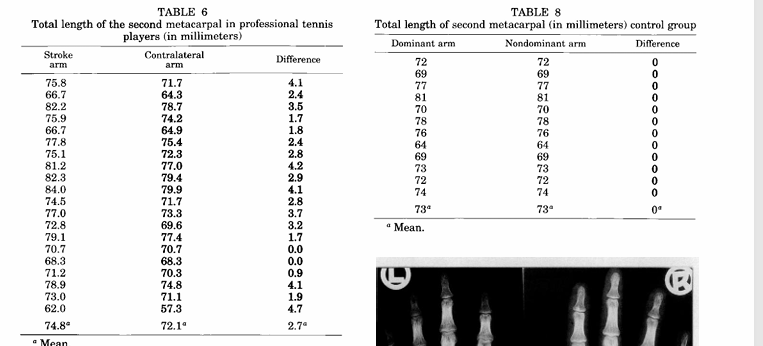
So there was a striking difference in the length of the ulna in professional tennis players and almost no different in control individuals.
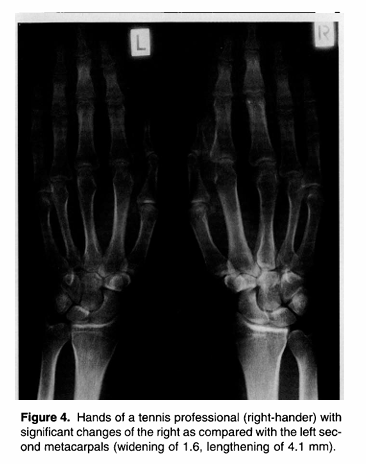
So note that the metacarpal is what increased in length which is a part of the palm. In testing, the palm tends to be what lengthened in our testing.
“Any stroke will transmit mechanical stimuli (vibrations) from the racket to the hand. Because the absorption of these vibrations by the racket is very slow, most of them have to be absorbed by the hand”<-note that vibration is outright mentioned as a possible means behind the lengthening in this paper. We are currently testing vibration in combination with other methods to induce lengthening. I do not believe vibration alone can lengthen bone.
“The second factor seems to be a temporary hyperemia of the muscular system of the dominant arm in tennis players that is induced by sports-specific strain.”
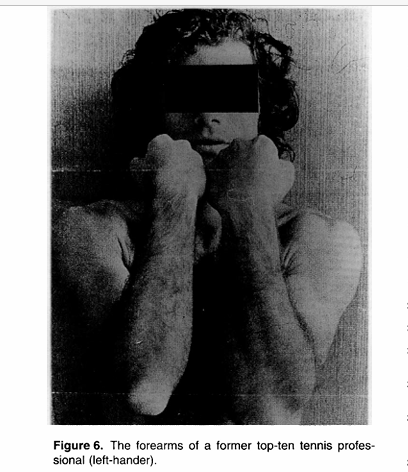
You can see below the major difference in length between a tennis players arms
Below you can see that the metacarpal increase in length in the tennis group but not the control group:
So the key takeaways for the study are that tennis can increase bone length. However, this increase was all pre skeletal maturity but there are other studies that show increase past skeletal maturity. Including anecdotal cases. This still gives credence to the fact that the forces induced by tennis can induce lengthening. I believe that these forces are torsion, vibration, and inversion/eversion of the arm against gravity.
Here’s a statement from a paper that cites the above one called The bone remodelling cycle. “The majority of bone modelling is completed by skeletal maturity but modelling can still occur even in adulthood such as in an adaptive response to mechanical loading and exercise and in renal bone disease.”<-It is possible that this bone modeling could increase length if the stimulation is strong enough. The loads for the arms are superior for those in the legs which is why we tend to see anecdotal cases of lengthening in the arms and not the legs. Arms invert and evert all the time but this is much rarer in the legs for example. You only see inversion/eversion during for example hamstring curls or kicks. We move our arms in a much more dynamic fashion than legs in general. we also experience greater torsion on the arms than the legs. Think hammer curls for example. However, vibrational forces are about equal on the arms and legs.