
This post is one of the final studies which sort of culminates the type of research where we look at the ability modern science and technology have been able to come to find a way to repair, regenerate, and completely grow cartilage to be used for repair and implantation and transplantion using the gene therapy method.
Note: The study below is missing the references and citations, which is critical to possibly find other critical studies. I intentionally left out the really long list of references. Please use the link below to find what is needed.
Analysis & Interpretation
The study itself was to summarize the multiple ways medical researchers have tried to use gene therapy to heal articular cartilage defects. As noted from previous posts, the two main ideas was always to either inject the adenoviral vector with the right type of growth factors inside directly to the defect area or close to it, or to go the second path to first inject the vector into progenitor cells which will be altered to express more chondrogenic differentiation. The stem cells are then injected and implanted to the cartilage area. While the main issue had been that the cartilage that was formed was fibrocartilage, the noticing of hyaline cartilage makes the venture seem even more likely to have great effectiveness.
The researchers note that any damage to articular cartilage means that it becomes hard to repair. The articular cartilage has a strong resistance from becoming vascularized, which suggest that if a damage does occur, there is not blood vessels to transport the needed tissue repair elements needed to the right area. It seems that nutrients in the hyaline cartilage matrix might actually be diffused to the chondrocytes. When there is a partial defect, that area does not get healed from there being no way for the healing elements to reach the ara of the defect. When there is a more serious defect in the articular cartilage, where the fracture or defect goes deeper and actually makes a cut or puncture in the chondral bone in the subchondral layer, the result is cartilage forming elements do come out of the inside of the bone but the cartilage they form is fibrocartilage, which has collagenous fibers that are not organized like hyaline cartilage.
When however not even the fibrocartilage is formed, that lead to pain for the subject so the medical professional might choose to stimulate the fibrocartilage formation process by doing a surgical technique known as abrasion anthroscopy, drilling, or microfracture surgery. The technique is reasonable effective and successful in removing the pain however it is well known that fibrocartilage is just not as good as the hyaline cartilage in the articular cartilage. There is much more Collagen Type 1 (while we are looking for Collagen type 2), there is more disorganization, etc. The result is that medical researchers have tried transplanting periosteum, perichondrium, and osteochondral parts to see what would happen .The short term effects is good in showing effectiveness in producing the hyaline cartilage they are looking for but the long term effects are not well known. It is suspected that one of the major problems is that there is not enough say periosteum or perichondrium available if a articular cartilage defect becomes too large.
The researchers seem to solve this problem by stating ,” Therefore, the autologous chondrocyte transplantation (ACT) procedure has been used clinically since 1987 in combination with a periosteal cover to treat chondral or osteochondral defects of the knee with good clinical results”
The top phrase means that the main way the researchers do it is to put the chondrocytes they get from an explant into a solid matrix (like a scaffold) and then implant the matrix which has the chondrocytes inside. Like one will learn from the Wikipedia article on the basic steps of Tissue Engineering, this is what tissue engineering is completely about. The result is that the symptoms in terms of pain does go away, at least for a short time while there is the autologous chondrocyte implant. However, again we see that the formation of really durable hyaline cartilage tissue is hard to form.
The whole point of the researchers can be summed up by their next sentence, “Therefore, tissue engineering approaches are being aggressively investigated in an effort to engineer cartilage in vitro to produce grafts to facilitate regeneration of articular cartilage in vivo“
The steps the researchers almost always goes through is…
- The original chondrocyte cells or progenitor mesenchymal stem cells are taken from some enzymatic digestion process or an outgrowth culture.
- The cells are put in a culture where they are slowly grown to increase in number until a cell colony (or sufficient cell number density) is formed.
- The cells are then injected in a a scaffold or matrix because you need something to hold the chondrocytes in place for a 3-D space.
- The matrix is then injected with growth factors to further grow the cell numbers and cartilage formation.
- The matrix is then implanted into the cartilage defect.
The problems on why this general step by step procedure don’t seem to work well in new hyaline cartilage formation are…
- insufficient differentiation
- loss of transplanted cells or tissues
- matrix destruction
- integration failures
In the next section the researchers show that all of these problems which have been inhibiting the formation of new hyaline cartilage has been themselves been inhibited or have their inhibitory effects mostly stunted. There are now…
- morphogens and transcription factors that promote differentiation along chondrogenic lineages – thus solving the differentiation problem
- growth factors that promote matrix synthesis – thus solving the matrix destruction problem
- inhibitors of osteogenic or hypertrophic differentiation – it helps reduce the integration failures since it prevents osteogenic tissue from appearing, letting the chondrogenic tissues have a chance to form before being cut off by the bone making elements.
- antagonists that inhibit apoptosis – thus solving the loss of cells problem
- senescence or responses to catabolic cytokine – which solves the loss of tissues and cells problem
However even this new ideas and ways have their own set of problems. Those problems would be…
- delivery problems
- the limited half-life of many of the proteins that might be injected in vivo
- the difficulty in administration of the elements at a high enough concentration and for a long enough time for effectiveness
- the injected material can also affect non-targeted tissue and organs.
As a consequence, the researchers felt that it would be much more effective in use a gene therapy approach. The best approach would be to be able to alter the genetics of the chondrocytes close to the defect so that any type of hyaline cartilage regeneration will be more natural instead of trying to embed a transplant.
From Table 1 there will be a list of candidates to be put into a vector including all the types of TGF-Beta, IGF-1, BMPs, FGFs, and EGFs. The IHH, SHH, SMAD, and Sox genes are also named as potential regulators for chondrogenesis. Some of these components can be combined together to have a more effective regulatory role.
“There are many strategies that can be used to deliver exogenous cDNAs for the treatment of diseased or damaged cartilage….A key component for any gene therapy application is a vector that efficiently delivers the cDNA of interest to the target cell, and enables transgene expression of a suitable level and duration to affect the desired biological response. Furthermore, an understanding of the natural behavior of the target cell, such as its half-life, rate of division, and infectability with the vector are also essential to the effectiveness of the procedure.”
The basic principle of gene therapy is explained again. You put the cDNA into a vector, you inject the vector into a cell to change the way the DNA inside the cell to express genes in terms of types and amount. So far the ways gene therapy has been used in tissue engineering range from being the most complicated to being the simplest.
As we have said before, there is two main ways for vector use in intra-articular cartilage repair, the in vivo method and the ex vivo method. The in vivo method means putting the vector directly on the defect. The ex vivo method means putting the vector into cells first , and then transferring the cells to the defect. Which type of method to use depends on the gene being delivered and the vector to be used.
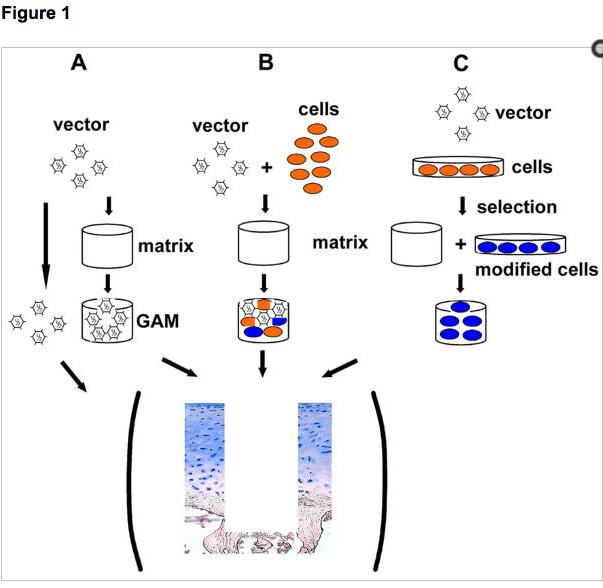 After this, the researchers would go into explain the 4 main ideas expressed in the diagram to the left.
After this, the researchers would go into explain the 4 main ideas expressed in the diagram to the left.
They are …
Gene transfer to the synovium – add the vector to the synovium cells
Gene transfer to the cartilage defect – add the vector to the cartilage defect area for local trans-expression of the desired results from the chondrocytes in the area
Gene transfer to the chondrocytes – add to chondrocytes
Gene transfer to the mesenchymal stem cells – Note what the researchers said about the MSCs approach, “However, a successful use of MSCs to aid cartilage repair by means of generating a stable hyaline-rich cartilage repair tissue in vivo, likely requires the efficient delivery of factors to stimulate MSCs toward chondrogenesis, and maintenance of an articular cartilage phenotype without ossification, fibrinogenesis, or inflammation”
Implications For Height Increase
I think it is time to move our scope of analysis out more and see the forest and not the trees. We’ve gone really technical and deep into the details of this idea of gene therapy for intra-articular cartilage repair and we have to ask ourselves how we can use it to increase height. It has come to my awareness that the key to being able to say create a pseudo-growth plate after the natural growth plates close was to study the current medical science on how to regrow cartilage, but more specifically the hyaline cartilage. The best idea would be to create new epiphyseal cartilage, but the stacking nature of the chondrocytes to get the columns is something I still haven’t found much details on. There was only one study which showed that a chemical compound seems to result in the columnar arrangement of the chondrocytes. At this point I am just trying to study more on the way gene therapy works, on how tissue engineering works, and how the articular cartilage can possibly be regenerated after defects are formed. If this area of research is understood as a deep enough level then we can propose a way to using just a few injections get a part of the long bones to start creating hyaline cartilage. My theory is that as long as we can get hyaline cartilage (and maybe even fibrocartilage0 to be formed in a way that makes the tissue go completely around the cortical bone area, then we can use other methods like mechanical loading to get the bone to be lengthened with relative ease.
I had proposed many idea in the past on how to alter the bone and the cartilage in the long bone for increased length before using ideas like autologous chondrocyte transplantations, but the ideas were still only relatively vague and the details were missing. With this study I would be able to develop a more coherent and scientifically sound idea on how to use tissue engineering and gene therapy for cartilage regeneration for longitudinal increase in the long bones.
Note: The full study is copy and pasted below for reference if one desires to see the original paper.
doi: 10.1016/j.injury.2008.01.034
Once articular cartilage is injured, it has a very limited capacity for self-repair. Although current surgical therapeutic procedures to cartilage repair are clinically useful, they cannot restore a normal articular surface. Current research offers a growing number of bioactive reagents, including proteins and nucleic acids, that may be used to augment different aspects of the repair process. As these agents are difficult to administer effectively, gene transfer approaches are being developed to provide their sustained synthesis at sites of repair.
To augment regeneration of articular cartilage, therapeutic genes can be delivered to the synovium, or directly to the cartilage lesion. Gene delivery to the cells of the synovial lining is generally considered more suitable for chondroprotective approaches, based on the expression of anti-inflammatory mediators. Gene transfer targeted to cartilage defects can be achieved by either direct vector administration to cells located at or surrounding the defects, or by transplantation of genetically modified chondrogenic cells into the defect. Several studies have shown that exogenous cDNAs encoding growth factors can be delivered locally to sites of cartilage damage, where they are expressed at therapeutically relevant levels. Furthermore, data is beginning to emerge indicating, that efficient delivery and expression of these genes is capable of influencing a repair response toward the synthesis of a more hyaline cartilage repair tissue in vivo. This review presents the current status of gene therapy for cartilage healing and highlights some of the remaining challenges.
Introduction
The application of gene transfer to articular tissues was pioneered by Evans and co-workers, as a means to treat arthritis [46,49]. Initial encouraging experiments in animal models using retroviral-mediated gene delivery formed the basis for a clinical trial to evaluate the safety and feasibility of using gene therapy for rheumatoid arthritis [46,49,59-61,148]. The study was completed without incident; the procedure was well-tolerated by the nine participants, and intra-articular gene transfer and expression was observed in all joints treated [46,49]. The relative success of these studies suggests that this technology may have application in treating a number of articular disorders for which current treatment modalities are unsatisfactory. Compared to the treatment of chronic or genetic diseases, where likely a lifelong expression of a corrective transgene is required, the use of gene transfer techniques to facilitate musculoskeletal tissue repair offers perhaps an immediate opportunity for a clinical application of gene therapy, as it may only require transient, localized expression of a specific transgene product. Whereas good success has been achieved by gene transfer to bone healing [9], augmenting the repair of focal articular cartilage defects by gene transfer has not been straightforward. Current research indicates that the design of a successful genetic approach for cartilage repair includes a refined strategy of gene delivery that meets the complexities of treating this tissue. This review aims to summarize some of the basic principles of cartilage injury and regeneration, and comments on the pros and cons of recent gene therapy approaches to repair, as well as future challenges.
Cartilage injury and limitations of current treatments
Hyaline articular cartilage is a highly specialized tissue that protects the bones of diarthrodial joints from forces associated with load bearing, friction and impact. Although a remarkably durable tissue, once articular cartilage is injured, it has very limited capacities for self-repair. In partial thickness defects, where a lesion is wholly contained within the articular cartilage, there is no involvement of the vasculature. Consequently, chondroprogenitor cells in blood and marrow cannot enter the damaged region to influence or contribute to the reparative process. Resident articular chondrocytes do not migrate to the lesion, and production of a reparative matrix by these cells does not occur. As such, the defect is not filled or repaired and essentially remains permanently [21,80]. Full thickness cartilage injuries result in damage to the chondral layer and subchondral bone plate, causing rupture of blood vessels, and hematoma formation at the injury site. In this case, a repair response is initiated that results in the formation of a fibrocartilage repair tissue within weeks [21,80].
In focal cartilage defects, where a stable fibrocartilaginous repair tissue has not formed, and patients are suffering clinical symptoms such as pain and swelling, surgeons aim to promote a natural fibrocartilaginous response, by using marrow stimulating techniques, such as abrasion arthroplasty, Pridie drilling, or microfracture. These procedures are cost effective and clinically useful, as patients often have reduced pain and improved joint function, and are therefore generally considered as first-line treatment for focal cartilage defects [22,121,122,161,162]. However, fibrocartilage has inferior mechanical and biochemical characteristics compared to normal hyaline articular cartilage. It is poorly organized, contains significant amounts of collagen type I, and is susceptible to injury. The inferior repair matrix breaks down with time and loading, which ultimately leads to premature OA [21,80]. Therefore, as outlined in other articles of this issue, the aim of modern therapeutic techniques is to achieve a more hyaline-like cartilage repair tissue by transplanting tissues or cells. Tissue transplantation procedures such as periosteum, perichondrium, or osteochondral grafts have shown positive short term results for a number of patients, but the long term clinical results are uncertain, with tissue availability for transplant being a major limitation, especially in large cartilage defects [19,22,23,71,80]. Therefore, the autologous chondrocyte transplantation (ACT) procedure has been used clinically since 1987 in combination with a periosteal cover to treat chondral or osteochondral defects of the knee with good clinical results [20,121,144,145]. Modern modifications of this procedure include embedding chondrocytes in a three dimensional matrix before transplantation into cartilage defects [15,114,123]. Despite these advances, most surgical interventions only result in improvement of clinical symptoms, such as pain relief, but none of the current treatment options has regenerated long-lasting hyaline cartilage repair tissue yet [22,80,121,144]. Therefore, tissue engineering approaches are being aggressively investigated in an effort to engineer cartilage in vitro to produce grafts to facilitate regeneration of articular cartilage in vivo. In most cases, cells are harvested by enzymatic digestion or outgrowth culture, which are thereafter extensively expanded in culture. The cells are then seeded onto various biologically compatible scaffolds, and cultured in the presence of a specific cytokine or growth factor, or a cocktail of bioactive factors. However, despite promising in vitro data with several approaches, a significant improvement compared to current cartilage repair modalities, has yet to be achieved. Many challenges thus remain for successful cell-based cartilage repair approaches to form hyaline repair tissue in vivo [23,80,92,177]. Impairments of hyaline neo-cartilage formation is likely due to a number of reasons, including insufficient differentiation, loss of transplanted cells or tissues, matrix destruction and integration failures, which all can occur due to various reasons.
Candidate gene products
In recent years, several factors have been identified that might be functional in augmenting different aspects of cartilage tissue repair. Of particular interest are morphogens and transcription factors that promote differentiation along chondrogenic lineages, growth factors that promote matrix synthesis, inhibitors of osteogenic or hypertrophic differentiation, antagonists that inhibit apoptosis, senescence or responses to catabolic cytokines (Table 1). Several of these substances have shown promise in animal models of cartilage repair and regeneration, but their clinical application is hindered by delivery problems [103,164,171]. Due to the limited half-lives of many proteins in vivo, they are particularly difficult to administer to sites of cartilage damage at therapeutic concentrations and for sustained periods of time. Localized delivery of these agents without involvement of non-target organs has also proven to be problematic [164,171]. We suggest that these limitations may be overcome by adapting appropriate gene transfer technologies. In particular, it should be possible to develop techniques for transferring therapeutic genes encoding the necessary gene products to cells at the sites of injury or disease, for sustained local expression at high levels with minimal collateral exposure of non-target tissues [164,171]. In this manner, the proteins of interest are synthesized locally by cells and are presented to the microenvironment in a natural fashion. Furthermore, recombinant proteins produced by overexpression in bacteria may have altered activity, since they may not be similarly modified post-translationally as when synthesized by a mammalian cell [113].
The list of potentially useful cDNAs for cartilage repair (Table 1) comprises members of the transforming growth factor (TGF)-β superfamily, including TGF-βs 1, 2, and 3, several of the bone morphogenetic proteins (BMPs), insulin-like growth factor (IGF)-1, fibroblast growth factors (FGFs), and epidermal growth factor (EGF), among others (reviewed in [74,103]). Other secreted proteins, such as indian hedgehog (IHH) or sonic hedgehog (SHH), play key roles in regulating chondrocyte hypertrophy [185], and may also prove to be beneficial for modulating the chondrocytic phenotype of grafted cells. Another class of biologics that may be useful in cartilage repair is transcription factors that promote chondrogenesis or the maintenance of the chondrocyte phenotype. SOX9 and related transcription factors like L-SOX5, and SOX6 have been identified as essential for chondrocyte differentiation and cartilage formation [98]. Signal transduction molecules, such as SMADs, are also known to be important regulators of chondrogenesis [76]. As these molecules function completely intracellularly, they cannot be delivered in soluble form, and gene transfer might be the only way to harness these factors for repair. Alternatively, delivery and expression of cDNAs encoding specific extracellular matrix (ECM) components such as collagen type II, tenascin, or cartilage oligomeric matrix protein (COMP), may also be used to support production and maintenance of the proper hyaline cartilage matrix [37].
Prevention or treatment of cartilage loss may also require the inhibition of the actions of certain pro-inflammatory cytokines, such as interleukin (IL)-1 and tumor necrosis factor (TNF)-α, as these are important mediators of cartilage matrix degradation and apoptosis after trauma and disease. Therefore, anti-inflammatory or immunmodulatory mediators, such as interleukin-1 receptor antagonist (IL-1Ra), soluble receptors for TNF (sTNFR) or IL-1 (sIL-1R), IL-4 or IL-10, inhibitors of matrix metalloproteinases, and others may be administered to effectively reduce loss of repair cells and matrix [148].
Inhibitors of apoptosis or senescence, such as Bcl-2, Bcl-XL, hTERT, i(NOS) and others (Table 1), may also be beneficially employed in order to maintain cell populations at the injury site, which are capable of favorable repair responses [39,41]. Different candidate cDNAs might also be administered in combination, especially when favoring complementary therapeutic responses. For example, the combined administration of an anabolic growth factor (e.g. IGF-1) together with an inhibitor of the catabolic action of inflammatory cytokines (e.g. IL-1Ra) has the potential to control matrix degradation as well as to allow partial restoration of the damaged cartilage matrix [73,132].
There are many strategies that can be used to deliver exogenous cDNAs for the treatment of diseased or damaged cartilage. For a successful approach, several factors have to be taken into account, including the extent of cartilage pathology, disease processes, and the biological activity of the gene product, among others. A key component for any gene therapy application is a vector that efficiently delivers the cDNA of interest to the target cell, and enables transgene expression of a suitable level and duration to affect the desired biological response. Furthermore, an understanding of the natural behavior of the target cell, such as its half-life, rate of division, and infectability with the vector are also essential to the effectiveness of the procedure. The properties of commonly used vectors in gene therapy applications are summarized in Table 2, and have been extensively reviewed elsewhere [136,168]. Gene-transfer strategies in which these vectors are currently used for cartilage repair, range from those as simple as direct delivery of a vector to a defect, to synthesis of cartilaginous constructs through genetically augmented tissue engineering procedures. We will present below an overview on the properties of commonly used vectors in gene therapy applications (Table 2), and will discuss their use in the context of the different delivery strategies to cartilage defects.
There are two general modes of intra-articular gene delivery, a direct in vivo, and an indirect ex vivoapproach (Figure 1). The direct in vivo approach involves the application of the vector directly into the joint space, whereas the ex vivo approach involves the genetic modification of cells outside the body, followed by re-transplantation of the modified cells into the body. The choice of which gene transfer method to use is based upon a number of considerations, including the gene to be delivered, and the vector used. In general, adenovirus, herpes simplex virus, adeno-associated virus vectors, lentivirus and non-viral vectors may be used for in vivo and ex vivo delivery (Figure 1, Table 2). Retroviral vectors, because of their inability to infect non-dividing cells, are more suited for ex vivo use. Ex vivo approaches are generally more invasive, expensive and technically tedious. However, they permit control of the transduced cells and safety testing prior to transplantation. In vivo approaches are simpler, cheaper, and less invasive, but viruses are introduced directly into the body, which limits safety testing.

Toward the treatment of damaged articular cartilage, the three primary candidate cell types to target genetic modification are synovial lining cells, chondrocytes, and mesenchymal stem cells.
The simplest strategy for gene delivery to diseased joints is by direct intra-articular injection of a recombinant vector [60,61]. For this application, the two primary tissues to consider are cartilage and synovium. Within articular cartilage, chondrocytes are present at low density and reside at varying depths within the dense matrix. Because of this, efficient genetic modification of chondrocytes in situhas not been effectively achievable [32,62,170,192]. The synovium, in contrast, is a tissue that is much more amenable to gene delivery. It usually exists as a thin lining of cells that covers all internal surfaces of the joint except that of cartilage, and thus has a relatively large surface area, and is therefore the predominant site of vector interaction. Direct intra-articular injection of vector or modified cells results in synthesis and release of therapeutic proteins into the joint space, which then bathe all available tissues, including cartilage. Using various types of vectors in ex vivo and in vivo approaches, considerable progress has been made towards defining the parameters critical to effective gene transfer to synovium and prolonged intra-articular expression. The effectiveness of synovial gene transfer of various transgenes is well documented in research directed towards rheumatoid arthritis [148]. Ex vivogene delivery to joints has since been taken into phase I clinical trial and shown to be feasible and safe in humans with RA [46,50].
Although most of the work involving direct intra-articular gene delivery has been focused toward the study and treatment of RA, data are beginning to emerge of its potential for treating OA (reviewed in [47]), and to augment repair approaches of focal cartilage defects (Table 3) [31,58,164,171]. For example, encouraging results have been reported for adenovirally delivered IGF-1 or IL-1Ra using animal models for OA and localized cartilage injury [32,54]. While it is possible to achieve biologically relevant levels of transgene expression by both direct and ex vivo gene transfer to synovium, this approach is not compatible with the delivery of certain growth factors. For example, adenoviral mediated delivery of TGF-β1 or BMP-2 to the synovial lining was found to generate joint fibrosis, extreme swelling, osteophytes and cartilage degeneration [8,56,57,120]. Considering these results in the context of cartilage repair, synovial gene transfer may be more suitable for delivering chondroprotective agents rather than strong anabolic transgenes with pleiotropic effects of their products. Many anti-inflammatory cytokines have this property (see Table 1).
For the gene-based delivery of certain growth factors or intracellular proteins, a strategy whereby the transgenes are more localized, and the gene products contained within the cartilage lesion, appears to be most prudent. Possibly, the most direct manner by which to achieve this goal is by implantation of a three-dimensional matrix pre-loaded with a gene delivery vehicle into a defect, allowing infiltrating cells to acquire the vector and locally secrete the stimulating transgene products [18,48]. Genetically activated implants have been designed to augment the healing of bones, ligaments and also cartilage [17,34,48,140,141,150]. For example, hydrated collagen-glycosaminoglycan matrices containing adenoviral vectors have been found to promote localized reporter gene expression in vivo, following implantation into osteochondral defects in rabbit knees, for at least 21 days [140]. However, given the usually limited cell supply at the cartilage lesion site, it is not yet known whether this type of approach can induce a sufficient biological response for repair. In order to increase the cellularity of the graft, while preserving the feasibility of the procedure within one operative setting, the genetically activated matrix could be mixed together with autologous cells, which are intraoperatively readily available, e.g. cells from bone marrow aspirates (Figure 1). Such an abbreviated, genetically enhanced tissue engineering approach would thus save time and costs, while avoiding labor-intensive ex vivo culture of cells [48,140]. Their limitation, however, is the lack of control over gene transfer following implantation.
As there are several advantages, gene transfer has mostly been used to augment ex vivo cell delivery approaches for cartilage repair (Figure 1). Such an approach delivers a pure population of cells, that can be selected under controlled conditions; the graft is highly cellular, localizes transgene expression to the injury site without administration of free vector, and there is the possibility for safety testing prior to transplantation. In the context of ex vivo gene delivery to cartilage defects, several experimental studies have been performed, exploring gene transfer to chondrocytes or mesenchymal progenitor cells.
Gene transfer to chondrocytes
A major advantage of using autologous chondrocytes as cell source for cartilage repair is that their application has already found the way out of the experimental stadium to clinical practice [20]. In recent years, autologous chondrocyte transplantation (ACT) has become a clinically adopted procedure for cartilage defects, especially when marrow stimulation techniques failed to generate good clinical results [145]. In order to further improve the quality of the repair tissue, attempts have been made to enhance this procedure by the use of genetically-modified chondrocytes. Although chondrocytes have been somewhat resistant to transfection with plasmid DNA, certain lipid-based formulations have been found to enhance the efficiency of DNA uptake [106]. Viral based vectors, however, are capable of generating far higher levels of transgene expression with greater persistence. Monolayer expanded chondrocytes are readily transduced by viral vectors, such as Moloney Murine Leukemia Virus (MLV), lentivirus, adenovirus and AAV. Adenoviral-mediated delivery of various transgenes, such as TGF-β1, BMP-2 , IGF-1 or BMP-7, has been shown to stimulate the production a cartilage-specific matrix rich in collagen type II and proteoglycans, and a decreased tendency towards dedifferentiation [75,130,131,157,159]. Transfer of cDNA encoding matrix molecules, such as the collagen type II minigene, led to enhanced extracellular matrix production of human fetal chondrocytes [37]. Transduction with the transcription factor SOX-9 increased collagen type II expression of chondrocytes in three-dimensional culture in vitro [99,167], whereas overexpression of the transcription factor Runx-2 (Cbfa-1) stimulated chondrocyte maturation and induced a hypertrophic phenotype, expressing high levels of collagen types II and X, alkaline phosphatase and osteogenic marker genes [44,84].
Having shown that chondrocyte biology can be positively influenced by genetic modification, research focus has shifted towards their efficient delivery to cartilage lesions. The first approach would be the delivery of genetically modified chondrocytes in suspension. Several studies have shown that genetically modified chondrocytes are capable of expressing transgene products at functional levels following engraftment onto cartilage explants in vitro [42]. In such systems, genetic-modification with IGF-1 [107], FGF-2 [109], or SOX9 [33] led to significant resurfacing and thicker tissue enriched with proteoglycans and collagen type II, compared to transplanted control cells [106]. In addition, adenoviral-mediated IL-1Ra gene transfer to chondrocytes resulted in resistance to IL-1-induced proteoglycan degradation after engraftment [11]. As an alternative to delivery in suspension, efforts have also been made to augment tissue engineering procedures using genetically modified chondrocytes (Figure 1C). For this, the cells are transduced/transfected in monolayer and then seeded into a matrix for subsequent transplantation into chondral or osteochondral defects. In such three-dimensional culture systems, several transgenes have shown promising results in maintaining and promoting the chondrogenic phenotype in vitro, including TGF-β1, BMP-2, -4, -7, IGF-1, SOX9 among others [164,171,177].
Initial studies demonstrated that chondrocytes efficiently expressed reporter genes in chondral and osteochondral defects following genetic modifications with adenoviral, AAV, retroviral or plasmid vectors, and that transgene expression was prolonged for several weeks when the genetically-modified chondrocytes were seeded in three-dimensional matrices [12,82,89,108]. Results of efficacy studies are just beginning to emerge, showing the effects of genetically modified chondrocytes in cartilage lesions in vivo (Table 3). In an ex vivo approach, adenovirally-transduced chondrocytes expressing BMP-7 [75], incorporated in a matrix of autogenous fibrin, were implanted into full thickness articular cartilage defects in horses [75]. Four weeks after surgery, an increased tissue volume and accelerated formation of a proteoglycan and collagen type II rich matrix could be observed in the BMP-7 treated defects compared to control defects treated with irrelevant marker genes. However, after 8 months, the levels of collagen type II and proteoglycan, and the mechanical characteristics of the treated defects compared to the controls were similar. This was attributed in part to the declining number of allografted chondrocytes that persisted in the defects after 8 months [75]. Nevertheless, it is encouraging that genetically modified chondrocytes can be used to augment a cartilage repair process in a large animal model.
Gene transfer to mesenchymal stem cells
The use of autologous chondrocytes for the repair of articular cartilage is limited, as they have to be isolated from a very limited supply of healthy non-weight-bearing articular cartilage, which has to be surgically removed, with the risk of donor site morbidity. Furthermore, chondrocytes dedifferentiate during expansion with a subsequent loss of the chondrocytic phenotype. With regard to cell- and gene-based approaches to cartilage repair, mesenchymal progenitor cells, also referred to as mesenchymal stem cells (MSCs), provide an attractive alternative to chondrocytes. Although no clear phenotype has been described, through the use of the proper culture conditions, expanded MSCs can be stimulated to differentiate along specific pathways such as chondrogenesis, adipogenesis, and osteogenesis [23,25,26,28,86,92,134,135,146,175-177]. MSCs have been isolated from several sources, including bone marrow [147], trabecular bone chips [134], adipose tissue [198], periosteum, perichondrium and others, and have been shown to maintain their multilineage potential with passage in culture [195]. In order to harness MSCs for cartilage tissue engineering, analyses of the appropriate three-dimensional microenvironment to stimulate MSCs toward chondrogenesis in vitro und in vivo have been performed extensively, with factors such as TGF-β1, 2, -3, and BMP-2 emerging among the most popular candidates (see also Table 1). This research has led to the first clinical application of autologous bone marrow stromal cells for the repair of full-thickness articular cartilage defects in humans, which resulted in stable fibrocartilage tissue formation at the defect site [93,187]. However, a successful use of MSCs to aid cartilage repair by means of generating a stable hyaline-rich cartilage repair tissue in vivo, likely requires the efficient delivery of factors to stimulate MSCs toward chondrogenesis, and maintenance of an articular cartilage phenotype without ossification, fibrinogenesis, or inflammation [23,80,177].
In order to meet these requirements, gene therapy approaches hold promise for efficient implementation in cartilage repair procedures. In this context, MSCs are readily transduced by recombinant adenoviral, retroviral, lentiviral, AAV [24,57,195,196] and foamy viral vectors (A. Steinert and A. Rethwilm, unpublished observation). Specific liposomal formulations were used with some efficiency [69,106,107], as well as molecular vibration-based methods [160]. In vitro chondrogenesis has been shown, following plasmid-mediated BMP-2 and BMP-4 [1,163], retrovirus-mediated BMP-2 [27], and adenovirus-mediated BMP-13 gene transfer in the murine mesenchymal progenitor cell line C3H10T1/2. Marrow-derived, primary mesenchymal progenitor cells, genetically modified to express TGF-β1 or BMP-2, were also found to undergo chondrogenesis in aggregate culture, in contrast to IGF-1 modified cultures and reporter gene controls [196]. Interestingly, chondrogenesis in these cultures was also dependent on the level and duration of transgene expression and the viral load, indicating that these factors have to be carefully optimized for a successful in vivo translation of this technology [196].
Some first studies have been performed applying MSC-mediated gene delivery for cartilage repair in vivo. A variety of reporter genes have been successfully delivered to osteochondral defects via periosteal, perichondral or marrow derived MSCs [116,138,140,164,171]. Only a few studies have been conducted using therapeutic genes via MSCs thus far.
A genetically enhanced tissue engineering approach used constructs fabricated of retrovirally-transduced periosteal cells expressing BMP-7, which were seeded into polyglycolic acid scaffolds before transplantation into rabbit osteochondral defects [116,117]. The defects treated with BMP-7 modified progenitors revealed improved regeneration tissue of cartilage and bone, compared to controls after a maximum of 12 weeks post-implantation. In a study using a similar experimental approach, genetically modified periosteal cells transduced to express sonic hedgehog (SHH) were compared to the delivery of the BMP-7 cDNA, which resulted in a better overall repair of the SHH compared with the BMP-7 treated defects after 12 weeks postoperatively, and both were superior to marker gene controls [67]. Using the same animal model, constructs of a collagen type I hydrogel and marrow derived MSCs following liposomal GDF-5 (CDMP-1) gene delivery were shown to enhance cartilage repair compared with marker gene controls [90].
Another approach to study gene-induced chondrogenesis in vivo was devised by Gelse et al. who used gene transfer to MSCs for the repair of partial thickness cartilage lesions in rats [57]. The MSCs were isolated from rib perichondrium and, following adenoviral-modification with Ad.BMP-2 and Ad.IGF-1, delierved via a fibrin glue matrix to partial thickness cartilage lesions of the patellar groove. Both treatment with BMP-2 and with IGF-1 resulted in formation of improved repair tissue rich in collagen type II and proteoglycans, compared with the naïve and Ad.LacZ controls after 8 weeks [57]. However, the majority of BMP-2 treated joints showed signs of ectopic bone formation and osteophytes, which were not present in the knees of the IGF-1 treated defects [57].
In order to simplify elaborate and expensive ex vivo tissue engineering procedures, efforts are underway to facilitate gene delivery approaches to stimulate MSCs at the defect site in vivo toward chondrogenesis. The simplest way of achieving this aim is maybe via direct vector delivery to the cartilage defect site. Toward this end, direct application of recombinant AAV vectors in suspension [32], or of adenoviral vectors incorporated in hydrated collagen-glycosaminoglycan matrices [140] have been found to promote localized transgene expression within the repair tissue formed, following transplantation into cartilage lesions in vivo. However, considerable vector leakage to adjacent synovium was observed [140]. In an attempt to augment this kind of approach with an autologous cellular and space-filling entity, Pascher and colleagues demonstrated that when fresh bone marrow aspirates were mixed with a solution of recombinant adenoviral vectors and allowed to coagulate, MSCs within the coagulum acquired and expressed the transgene for several weeks after implantation into osteochondral defects in rabbits [140]. Studies are underway to investigate how these advances can be harnessed to achieve cartilage repair.
Currently used cartilage repair approaches, both experimental and clinical, are still far from generating a repair tissue that is comparable to the native cartilage tissue quality and stability. To tackle various obstacles toward successful repair, including matrix degradation, differentiation or integration insufficiencies, or loss of the transplanted cells and tissues, efficient delivery of chondrogenic, anti-inflammatory, and anti-oxidative factors seems to be crucial (Table 1). As most of these factors are recombinant proteins, which have short half lives, a repeated local administration is likely to be necessary to achieve the desired result, thus presenting delivery problems. Gene transfer techniques might be adopted that could overcome the limitations of the current treatments for damaged articular cartilage. The current concepts in gene therapy for cartilage repair are reviewed here. Various approaches have been shown to be suited for efficient transfer of exogenous cDNAs to cartilage defectsin vivo, and for achieving sustained expression of the corresponding gene products. Initial efficacy studies indicate that gene-transfer techniques are potent tools that can indeed stimulate a relevant biological response in vivo (Table 3). To date most approaches delivered a strong anabolic transgene aiming to achieve formation of a hyaline-like cartilage repair tissue in vivo, but with limited long-term success thus far. As more data surfaces, a clearer picture of the functional boundaries of current approaches appears. The future challenge therefore is to determine which combination of transgenes will be most suitable for which aspects of repair, and how best to deliver and express them.
Toward this end, the use of more refined vector systems seems to be crucial. Current gene transfer studies to cartilage repair have used vector systems with strong, viral-based promoters enabling very high levels of expression, thus facilitating study of the biological effects that may be achieved with a particular gene and gene delivery method. However it is likely that the stimulation of faithful synthesis of the complex architecture of articular cartilage, followed by its maintenance long-term will require the use of more sophisticated vector systems capable of coordinate control of expression. As many gene products proposed for use can have detrimental side effects if overexpressed in non-target organs such as the heart, lung or kidney, the characterization of the duration of expression in vivo and the biodistribution of vector and/or genetically modified cells following delivery, will be critical. Toward this end, there are several types of cartilage-specific regulatory elements that have been characterized and that might be incorporated into gene delivery systems, such as promoters for the cartilage-derived retinoic acid-sensitive protein (CD-RAP), the procollagen type II α1 (COL2A1), or the aggrecan gene [96,100,127,128,158,173,180,191,197].
Because cartilage injuries are not life-threatening, the safety of gene transfer approaches for repair is of particular importance. To harness the potential of this technology for clinical use is therefore strongly dependent on the use of safe and efficient vectors, transgenes and delivery systems.