How Yakson House Bone Setting Golki Therapy Massage Is Using Wolff’s Law To Change Facial Bone Shapes
 My recent interests have been moving towards looking into how some cultures have been using joint manipulation to help treat orthopedic conditions. I even went online and ordered two books.
My recent interests have been moving towards looking into how some cultures have been using joint manipulation to help treat orthopedic conditions. I even went online and ordered two books.
- Treatment by manipulation: A practical handbook for the practitioner and student – by A. G. Timbrell Fisher
- Manipulative surgery (Modern surgical monographs) – by A. S. Blundell Bankart
So far only the 2nd one came in. I took a picture of the book to show you guys just how old some of these early 20th century medical texts are. The book by Bankart was written back in the 1930s.
What I have found so fascinating about this non-invasive “surgical” way of treating joint mobility and pain problems back in the 1930s is that they seem to derive many of their knowledge from many other older cultures and medical traditions. I am reminded of what I found when I was searching to find out how many Malaysian, Singaporean, and Hong Kong Bone Setters are still left who has a vast knowledge on how to treat minor orthopedic problems just from hand manipulation. If you actually look at the Wikipedia article on the practice of “Bone Setting” you find out that almost all long standing ethnic groups have had some type of bone setter. If I was to take a guess, these bone setters would be maybe much better than the current chiropractors and people who do rolfing since the theory that they give on why the techniques of manual manipulation works is based on real anatomical facts.
In fact, if people ever did real research to see how modern Chiropractors explain why their techniques worked, they’d probably be very surprised to learn that the theory sounds very pseudo-scientific.
So I started to really look into how the various nations and cultures preform bone setting. That was how I came across this bone remodeling company based on Traditional Korean Medical techniques. You can read more on it from “Bone-setting: The new face of Korea“. The website is at Yaksom House. This 25 year old company seems to have at least 2 dozen offices around South Korea, and some in the Philippines, China, and now in NYC.
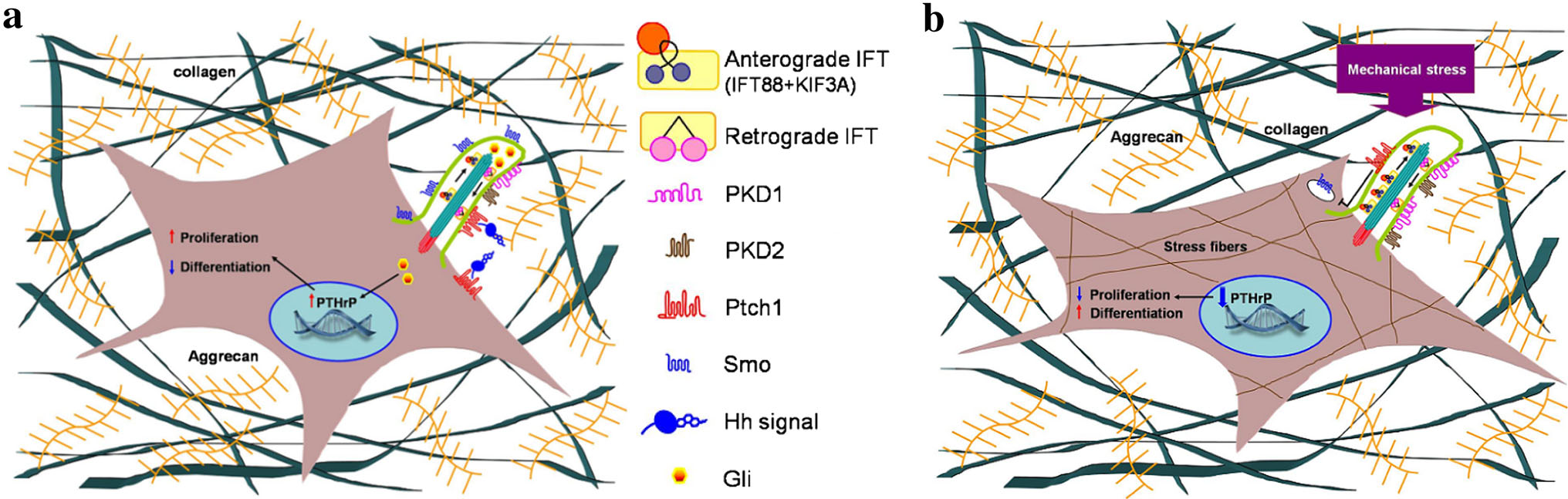
The explanation on how the facial bones can be remodeled they explain is due to Wolff’s Law, which we have talked about extensively on the website. The idea is that actual physical, mechanical stimuli to living bone would cause the local area of stimuli which is supposed to cause blood to increase in that area, which would as a result also lead to increased calcium absorption (or deposition). The increase in calcium absorption would make the bone thicker in that region.
I had theorized after reading Dr Becker’s Book on Bioelectricity that the real reason why Wolff’s law would ever work is that the physical stimuli causes electrons in other areas of the bone to be popped out of the atomic lattice and travel to the area of stimuli, and build up/accumulate. The result is that calcium ions, including calcium phosphate and calcium oxalate which are cationic (positive charge) start to go towards the now negatively charged location which is where the excess of electrons would be.
So does very strong, almost painful massages on one’s face really lead to thicker bone surfaces? In some ways it does.
However, the issue is that in Korean (and maybe most East Asian) culture, the desire for females is to have smaller faces to look more feminine. The main reason people go in for this Golki Therapy Massage is to make their faces smaller. It seems the primary foreign clients for the Korean based company is from Japanese women looking to have smaller faces. These asian women want smaller faces to look more attractive.
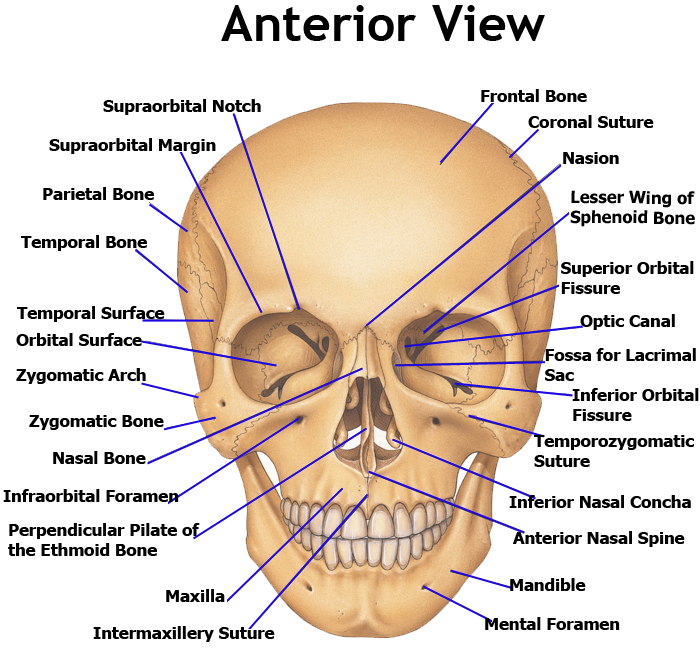 The truth is that I am not sure just how it is possible to make the faces of human beings smaller. Just like trying to pull bones longer when there is no cartilage between the bones, I am not sure how any human would be able to exert enough force to make fully ossified facial bones to become elastic and bend in the direction of applied force. I agree that if you look at enough skull bone arrangements you would see that the skull if not one large irregular bone that comes out fully formed, but in multiple parts which sort of fit together like a jig-saw puzzle. However, the adult human face has the bones almost completely fused together. (Picture source)
The truth is that I am not sure just how it is possible to make the faces of human beings smaller. Just like trying to pull bones longer when there is no cartilage between the bones, I am not sure how any human would be able to exert enough force to make fully ossified facial bones to become elastic and bend in the direction of applied force. I agree that if you look at enough skull bone arrangements you would see that the skull if not one large irregular bone that comes out fully formed, but in multiple parts which sort of fit together like a jig-saw puzzle. However, the adult human face has the bones almost completely fused together. (Picture source)
The human skull bones are over 1 cm thick, and the bones that make up the frontal side (ie zygomatic bone, maxilla, mandible) are also extremely thick, around 5-8 mm. This is the reason why you find that when guys are fighting and punch each other in the face, the only thing that is broken is the nose, because it is made of cartilage. Cartilage you can punch and break. Bones, not so much, (not without a bat, wrench, or something with much more hardness and force/per square inch, than most human fists). There is the temporozygomatic suture, which is the only place where you have any bone break but that is just one 1 mm thin line where the zygomatic bone meets the infraorbital foramen,, and there is the temporomandibular joint (TMJ), which you can kind of manipulate but those are really the only two places any person can move even slightly. There should not be any joints on the face which would be able to be elastic enough to make the base layer of bones smaller.
The effect of applying Wolff’s Law is in fact going to make the skull of the person getting the massager at least a few layers thicker aka slightly bigger, not smaller. However, what I suspect is happening is that the extremely strong massager is in fact kneading the skin and redistributing the collagen in the skin (Collagen Type I) around. The effect of very strong massages is that the collagen can be pushed thinner, and that is what is really happening. The facial bones are not getting thinner, but thicker. It is the skin layer which is getting thinner, since collagen can be manually moved around.
There will be indeed increased circulation, but there is already too many pseudo-scientific medical devices I’ve seen in the past year which claim some type of benefit from increased circulation. In fact, any time you break tissue and there is a rupture of capillaries, there an increase in circulating. Increased blood flow does not always means a good thing, although all cells in our body does require blood to flow pass them to get the oxygen and nutrients to diffuse to the cells for continued life.
In this case though, the massages are most likely relaxing to the person getting it, and does make the skin slightly better. The fact may be be shrinking aka remodeled but the person who comes out of these sessions probably do feel and look better.