Here’s the pictures of my fingers(you can follow the link on the page to get more images). I’ve been loading the right index finger with LSJL.
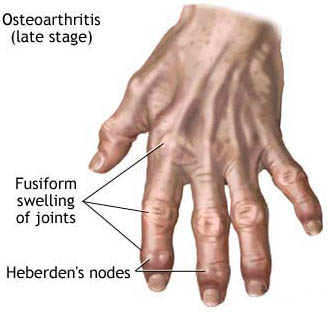
Here’s an image of osteoarthritis fingers:
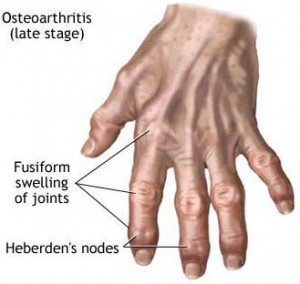 In contrast to heberden’s nodes my fingers are enlarged at the sides and there is no fusiform swelling of the joints. Fusiform swelling is ” elongated and tapering at both ends; spindle-shaped ”
In contrast to heberden’s nodes my fingers are enlarged at the sides and there is no fusiform swelling of the joints. Fusiform swelling is ” elongated and tapering at both ends; spindle-shaped ”
“Heberden’s nodes are hard or bony swellings that can develop in the distal interphalangeal joints (DIP) (the joints closest to the end of the fingers and toes). They are a sign of osteoarthritis and are caused by formation of osteophytes (calcific spurs) of the articular (joint) cartilage in response to repeated trauma at the joint.
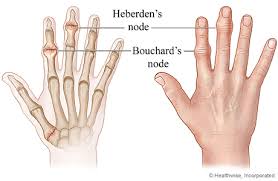
Heberden’s nodes typically develop in middle age, beginning either with a chronic swelling of the affected joints or the sudden painful onset of redness, numbness, and loss of manual dexterity. This initial inflammation and pain eventually subsides, and the patient is left with a permanent bony outgrowth that often skews the fingertip sideways. Bouchard’s nodes may also be present; these are similar bony growths in the proximal interphalangeal (PIP) joints (middle joints of the fingers), and are also associated with osteoarthritis.”
The question is, is my enlargement of the epiphysis of the fingers an osteophyte or is it a result of endochondral ossification. Although there are lateral osteophytes.
Heberden’s and Bouchard’s nodes
Osteophyte nodes may be painless so lack of pain in my fingers is not an indication that is not an osteophyte.
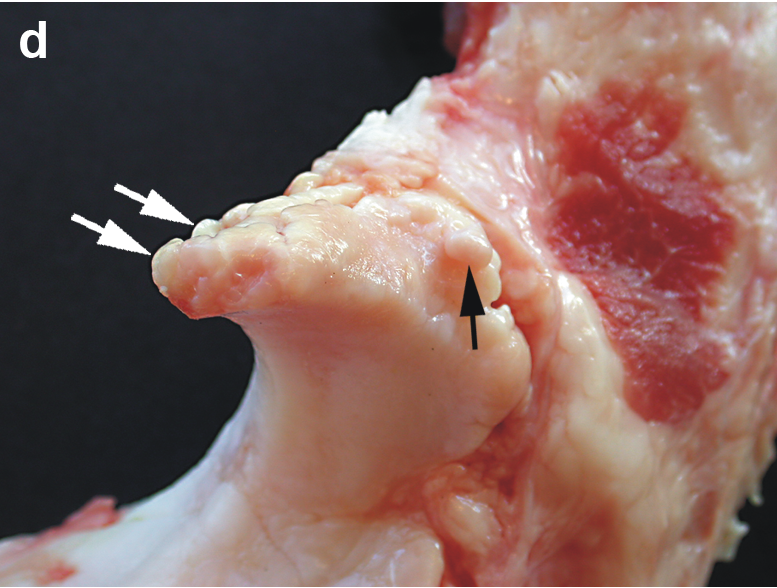
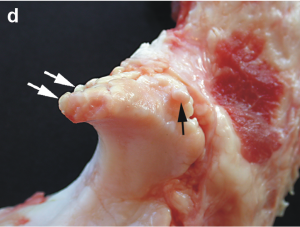
“The osteophytes beneath the lateral nodes arise lateral to the extensor tendon, and although the soft tissues have been distorted by the embalming process and have to be interpreted with caution, it appears that the adjacent capsule is displaced and attenuated.”
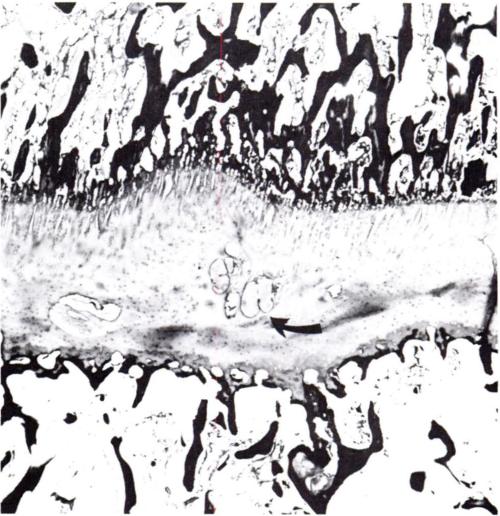
Here’s an image of a growing osteophyte:
 And admittedly this does appear to be like enlargement of the epiphysis.
And admittedly this does appear to be like enlargement of the epiphysis.
“The true osteophyte, initially a chondrophyte, is intra-articular, developing from the synovium covered surface at the cartilage margin, either from metaplasia of existing synoviocytes or differentiation of precursor cells. The chondral hyperplasia that initiates it is not intrinsically vectored to grow in any particular direction, and in practice grows in the direction of least resistance, to an extent determined by that resistance. If the adjacent cartilage surface is unloaded as a consequence of subluxation or underuse, the osteophyte will grow centripetally over the cartilage surface. More usually it grows peripherally, forming a large pedunculated osteophyte if unopposed, as in the synovial recess of the shoulder joint. Where growth is constrained by strong capsules, as in the lateral ankle, by adjacent ligaments as at the tibial spine, or by tendon insertions as in the upper humerus, growth is inhibited and the osteophyte is small. In essence it will grow until the tension induced in the stretched soft tissues matches that induced by the growing osteophyte. It follows from these known growth characteristics of osteophytes that the regular location of osteophytic nodes at specific sites in these two joints must reflect a local area of low resistance to osteophyte growth unique to these joints. ”
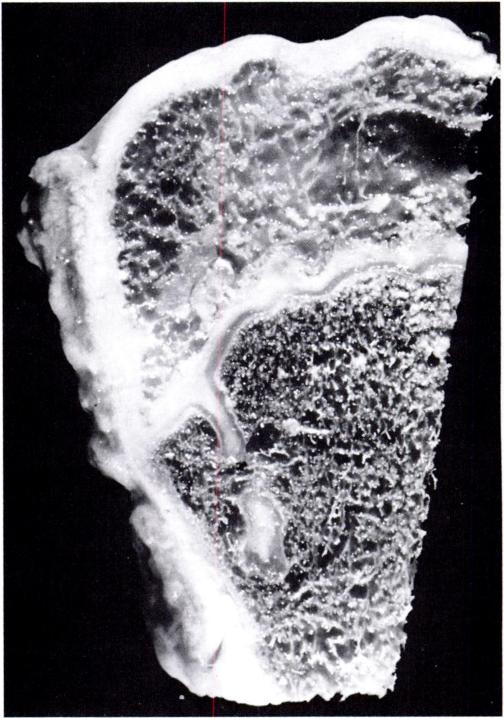
Here’s another image that better shows lateral nodes:
Here’s what an osteophyte looks like directly on the bone:
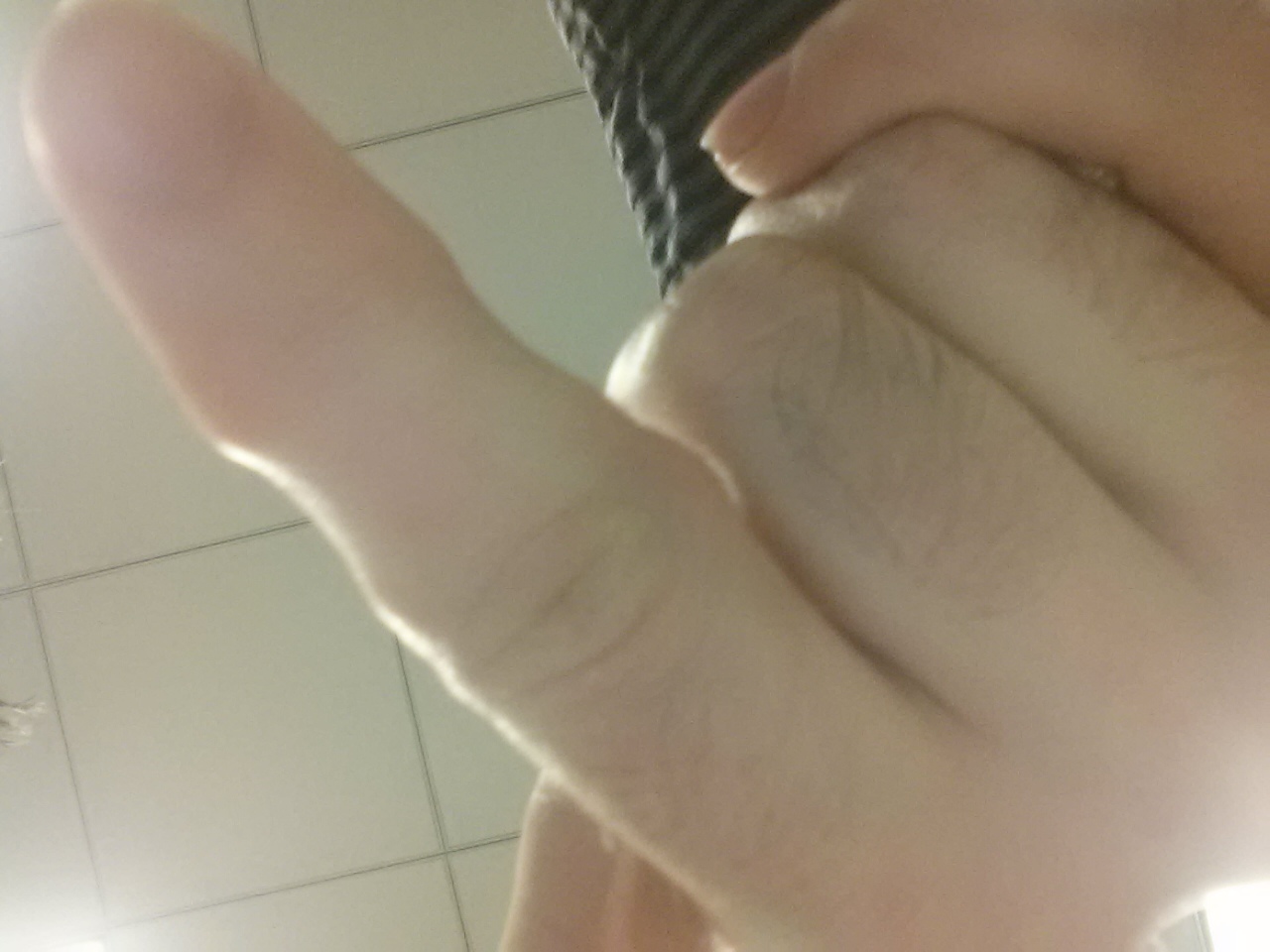
Now here’s another image of my loaded finger so you can see any potential osteophyte nodes:
 Definitely node like. I can’t see any evidence of swelling though. I’ve seen young people report getting finger nudes at like age 14 so arthritis may cause nodes but arthritis may not be the only source of nodes. And most evidence suggests that nodes aren’t painful and don’t limit mobility of the finger.
Definitely node like. I can’t see any evidence of swelling though. I’ve seen young people report getting finger nudes at like age 14 so arthritis may cause nodes but arthritis may not be the only source of nodes. And most evidence suggests that nodes aren’t painful and don’t limit mobility of the finger.
I couldn’t find any evidence upon searching that these nodes increase finger length although admittedly it is incredibly hard to use a search to find anything so that does not guarantee that there are not some anecdotal reports that people got longer fingers due to nodes.
So I conclude: LSJL caused increase in bone length and osteophytes and these two effects may be independent. I am using as much load as I can to get more finger results this may be overload and what is causing osteophytes. However, less load may be possible to increase finger length without causing osteophytes. I increased arm length with no evidence of osteophytes(unfortunately I did not document this).