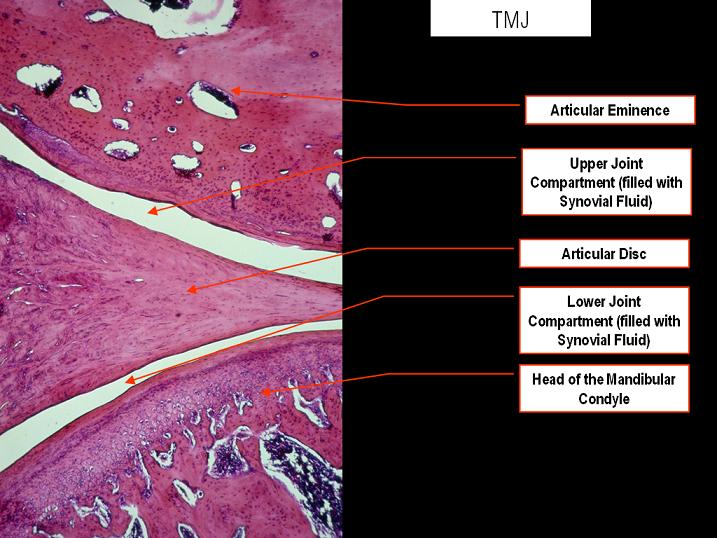
We’ve studied endochondral ossification of the articular cartilage in the condyle before. If vibration can induce endochondral ossification of the articular cartilage in the jaw it is theoretically possible that it could induce endochondral ossification in any joint unless the jaw cartilage is special. Which I don’t believe it is I believe that the jaw is more mobile than other joints and subjected to superior loading. If other joint regions were subjected to the same kind of loading as the jaw they could grow as well.
Effects of Mechanical Stimuli on Adaptive Remodeling of Condylar Cartilage
“Trabecular bone has been shown to be responsive to low-magnitude, high-frequency mechanical stimuli.
This study aimed to assess the effects of these stimuli on condylar cartilage and its endochondral
bone. Forty female 12-week-old C3H mice{this is pre skeletal maturity unfortunately, howver later in the study they say that the mice are “adult”} were divided into 3 groups: baseline control (killed at day 0), sham (killed at day 28 without exposure to mechanical stimuli), and experimental (killed following 28 days of exposure to mechanical stimuli).
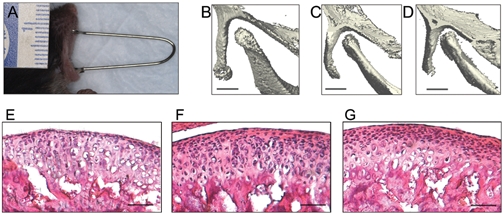
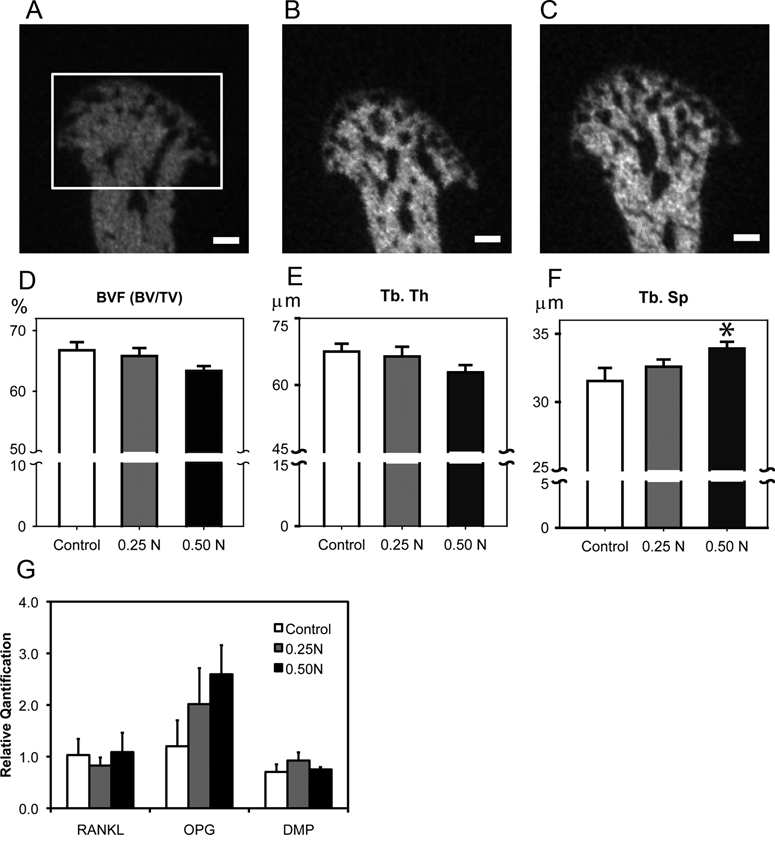
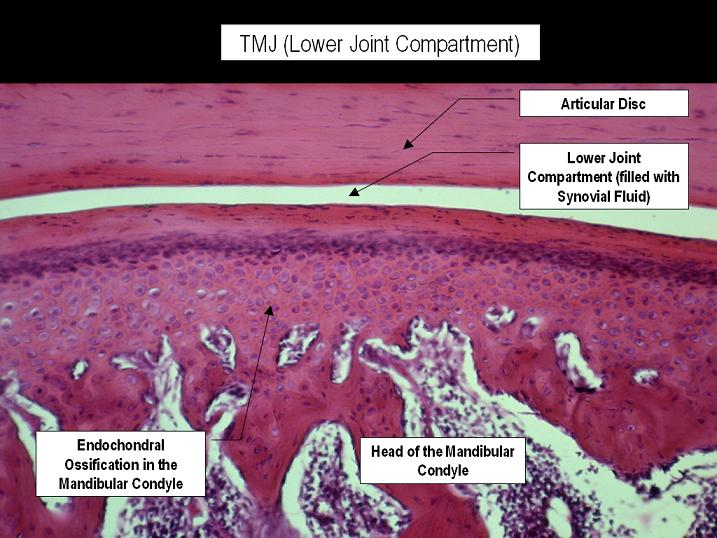
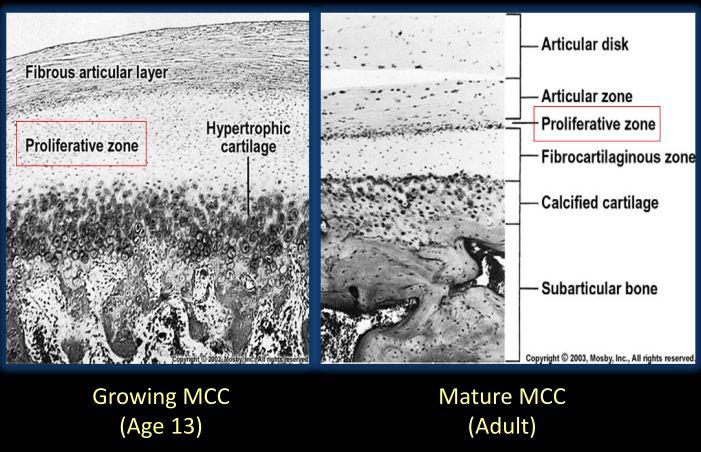
The experimental group was subjected to mechanical vibration of 30 Hz, for 20 minutes per day, 5 days per week, for 28 days. The specimens were analyzed by micro-computed tomography. The experimental group demonstrated a significant decrease in the volume of condylar cartilage and also a significant increase in bone histomorphometric parameters. The results suggest that the low-magnitude, high-frequency mechanical stimuli enhance adaptive remodeling of condylar cartilage, evidenced by the advent of endochondral bone replacing the hypertrophic cartilage{vibration can induce articular cartilage endochondral ossification, if this can occur in other joints with articular cartilage then you can get longer bones by that mechanism!}.”
“there is a linear association between bone-regenerative capacity and bone density”<-So could things that increase bone density increase bone regenerative capacity?
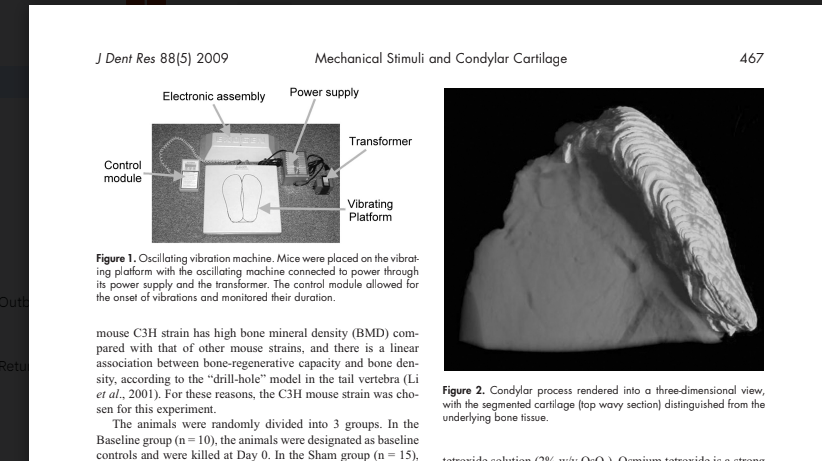
“We achieved mechanical stimulation to the animals by placing them, while still in their cages with bedding removed, directly on a device which generated vertical ground-based vibration. This machine generated 30-Hz pulses, creating peak-to-peak accelerations of 2.9 m/sec2, referred to as a fraction of earth’s gravitational field, 0.3 g (1g = 9.8 m/sec2). Based on Rubin’s previous research, it is believed
that this produces peak strains of approximately 5 μє. Animals in the Experimental group were subjected to 20 minutes’ vibration per day for 5 days per week for a total of 28 days,”<-so the mice were subjected to vibration not specific to the jaw and it still underwent articular cartilage endochondral ossification. It would be interesting if other bones changed as well.
“the LMHF stimuli induced osteogenesis, leading to adaptive growth of the condyle in adult mice.”<interesting that they call these adult mice! But we have to be sure they’re skeletally immature
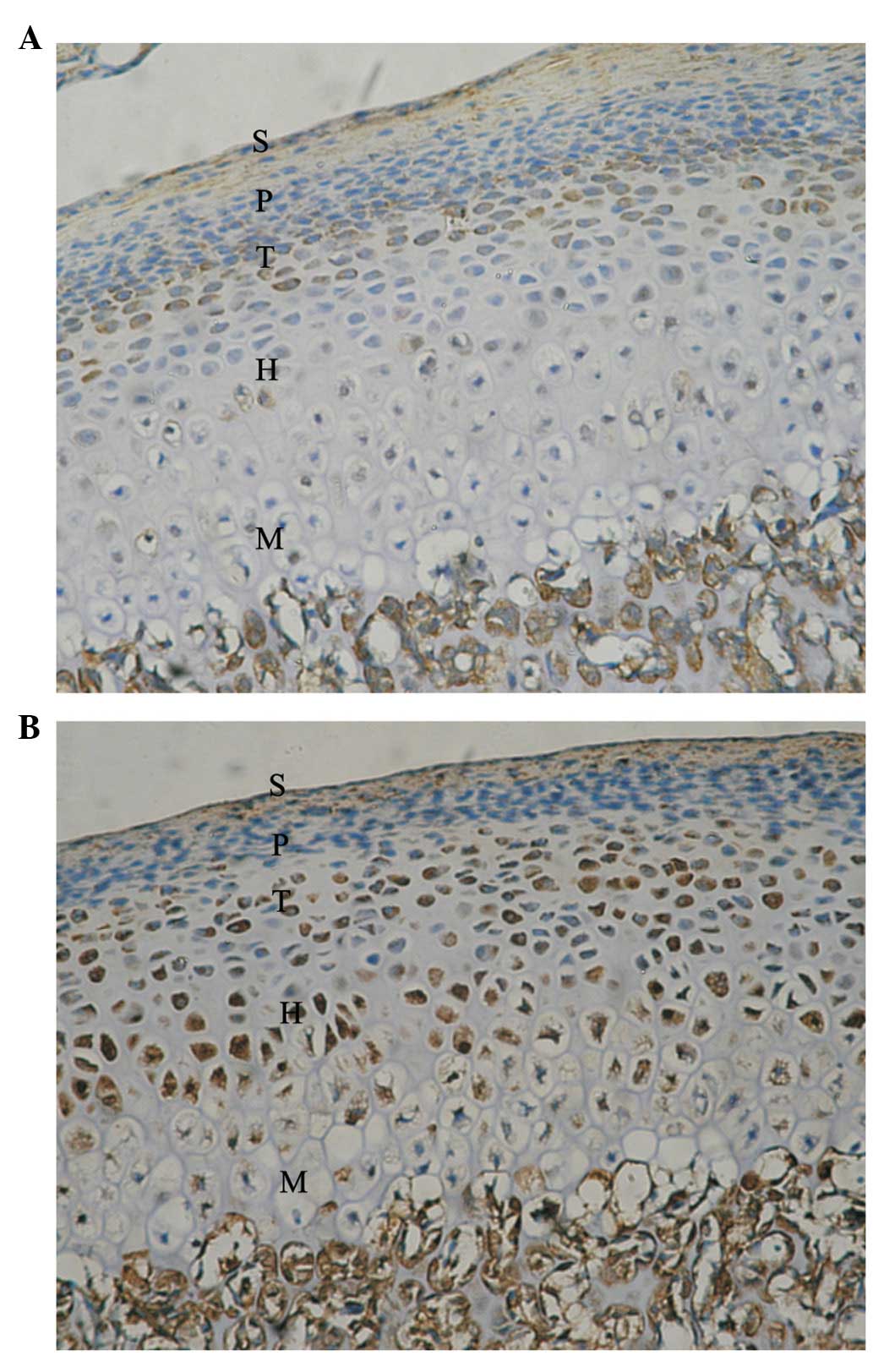
“the adaptive modeling of condylar cartilage is characterized by enhanced transition from chondrogenesis to osteogenesis. The vibrating mechanical stimulation in the present study was shown as a possible mechanism for the acceleration of the modeling.”
“A questionable aspect of this study design is the degree of transmission of the vertical ground-based oscillation, since it diminishes as the signal travels proximally through the skeleton. In a study measuring transmissibility in the hips and spines of humans standing on the oscillating plate, the authors showed
that approximately 80% of a 30-Hz ground-based signal reached the hip and spine”
This study here suggests that vibration can have benefit on growing bone:
Does Vibrational Loading Modulate the Effects of Radiotherapy on Growing Bone?
“[we evaluate] the possible beneficial effects of low-magnitude high-frequency mechanical vibration (LMHFV) stimuli on growing irradiated bone and the possibility for restoration of function of the epiphyseal plate”
“
ighteen 3-week old weanling male Sprague-Dawley rats were subjected to a standard radiation dose of 17.5 Gray applied to right hind limbs, with the contralateral leg serving as a non-irradiated control. Then, the animals were divided into three groups: A) rats subjected to (LMHFV) only at 45 Hz, 0.3 g for 20 minutes once per day, 7 days/week, for 3 weeks, B) rats subjected the same conditions of LMHFV plus an injection of spermine NONOate, a nitric oxide donor that that has shown weak positive results as post-irradiation recovery agent, and C) rats subjected to sham LMHFV. After euthanizing the animals, skeletal growth was measured by x-ray analysis, marrow mesenchymal stem cell osteoblastic potential was measured by CFU-F analysis, and bone morphology was measured by micro-CT analysis.
X-ray and CFU-F analyses show statistically significant differences between right and left limbs in all groups. No statistical significance was observed between vibration versus control groups, but trends suggest there could be some positive effect of vibration, although not statistically significant. Micro-CT results show a clear difference between right and left limbs in all groups. Regarding vibration versus control groups, micro-CT results are ambiguous, but do suggest that vibration may have altered local growth characteristics and stimulated local shape changes in the 20% region from the distal end of the femur, just above the growth plate.”
“Eighteen 3-week old weanling male Sprague-Dawley rats were obtained from Taconic Farms (Germantown, NY) and randomly divided into three groups: A) rats subjected to low-magnitude high-frequency vibration (LMHFV) only at 45 Hz, 0.3 g for 20 minutes once per day, 7 days/week, for 3 weeks, B) rats subjected to LMHFV with the same conditions as group A plus an injection of spermine
NONOate, a nitric oxide donor , and C) rats subjected to sham LMHFV, placed in cages
used for vibration but with no stimulus applied.”<-so we’re looking at group A versus group C as to whether vibration can increase bone length.
“there was possibly a difference, although not statistically significant, between right femora of different groups (A: 32.6±2.3 vs. B: 31.9±2.2 vs. C: 31.2±1.2, Figure 2), as well as total leg lengths of the femur
plus the tibia between different groups (A: 66.4±2.4 vs. B: 65.3±2.9 vs. C: 64.4±2.1, Figure 4).”<-So vibration group was longer than via group C.
“the ability of physical signals to influence bone morphology is strongly dependent on the signal’s magnitude, frequency and duration”