If it is possible to gain disc height by stretching. that could potentially explain the height gain of programs like agrobics. Unfortunately, this batch of research I found, does not produce a strong link between stretching and height gain. Mainly due to the nucleus pulposus being mechanically fragile.
The structural basis of interlamellar cohesion in the intervertebral disc wall.
“The purpose of this study was to investigate the structural mechanisms that create cohesion between the concentric lamellae comprising the disc annulus.”
” Additional bulk samples of annulus were fixed while held in a constant, radially stretched state in order to investigate the potential for interlamellar separation to occur in a state more representative of the intact disc wall. ”
“[IVD] tissues generally exhibit highly non-linear stress–strain responses, with the low-stress phase being a direct consequence of large-scale reversible alterations occurring in their fibrous architecture.”
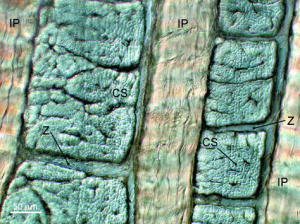
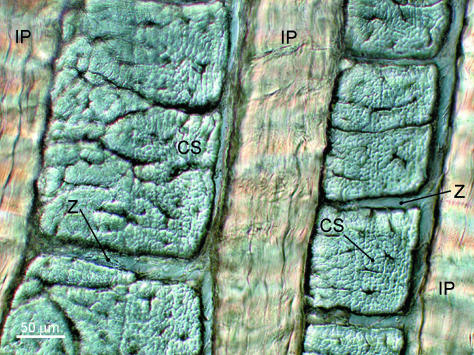
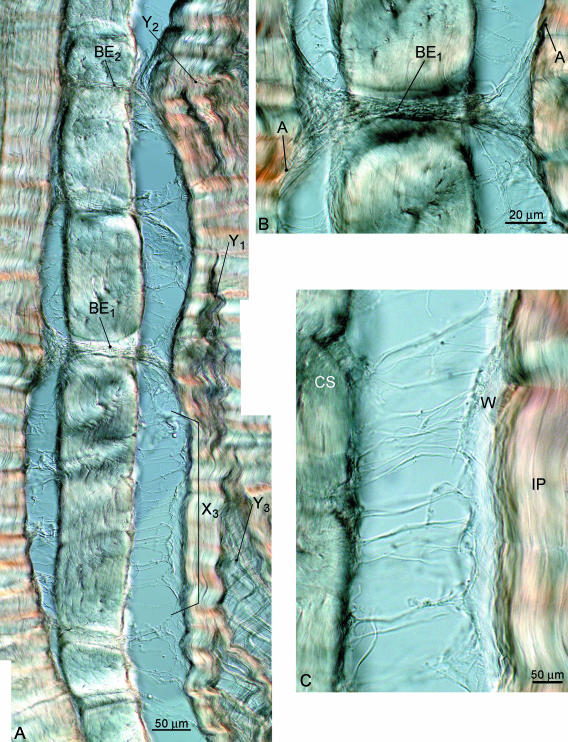
“Fully relaxed, hydrated interlamellar section showing adjacent lamellae as both in-plane (IP) and cross-sectioned (CS) arrays. Note the compartmental division between the cross-sectioned bundles at Z.”
 Here you can show the possibility that stretch can potentially lengthen the IVDS.
Here you can show the possibility that stretch can potentially lengthen the IVDS.

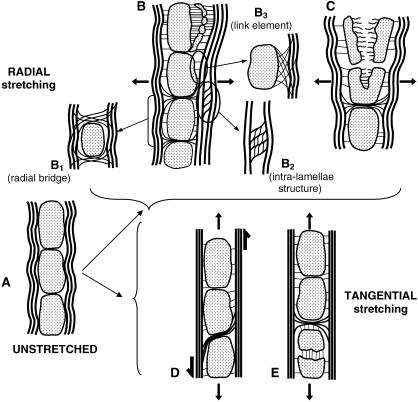
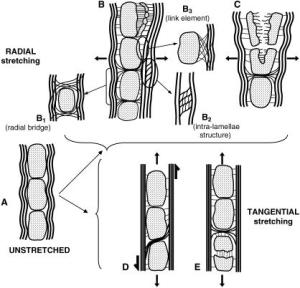
“(A) Interlamellar section subjected to radial stretching and revealing various modes of interconnection; (B) detail of radial bridging element passing between the cross-sectioned bundles; (C) detail of more uniformly distributed linking elements between adjacent lamellae.”<-This is radial stretching which should increase disc width rather than length.
“Interlamellar section radially stretching [causes] progressive fragmentation of cross-sectioned bundles ”
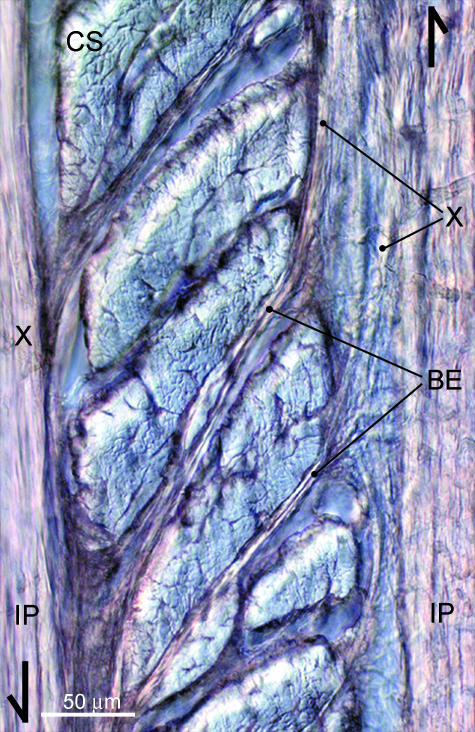
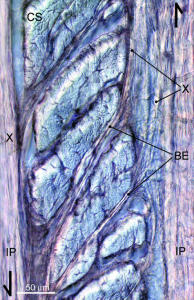 “Interlamellar section subjected to tangential stretching. Selective fibre bundle pullout at grip ends has induced a substantial degree of shear between the in-plane arrays, thus revealing further the extent to which bridging elements (BE) pass between the cross-sectioned bundles and connect the neighbouring in-plane arrays (IP).”<-So fibre bundles pull out and bridge elements form resulting in possible overall lengthening in response to stretching.
“Interlamellar section subjected to tangential stretching. Selective fibre bundle pullout at grip ends has induced a substantial degree of shear between the in-plane arrays, thus revealing further the extent to which bridging elements (BE) pass between the cross-sectioned bundles and connect the neighbouring in-plane arrays (IP).”<-So fibre bundles pull out and bridge elements form resulting in possible overall lengthening in response to stretching.
“With increased stretching the forces transmitted by these same interconnections resulted in a progressive fragmentation of the cross-sectioned bundles involved. [Fragments separate] from [their] parent cross-sectioned bundle (CS).”
“the overall morphology of the permanently stretched samples reveals a radial elongation of the cross-sectioned bundles”<-but this is disc width and not height.
This study illustrates a possible mechanism of increasing interverterbral disc height although it’s possible that disc height could be still limited by mechanisms not investigated in this study.
Here’s a study that investigates the effects of twisting directly on the entirety of the spine:
Low back pain development response to sustained trunk axial twisting.
“The trunk axial twisting was created by a torsion moment of 50 Nm for 10-min duration.”
“The results showed that there was a significant twist creep with rotational angle 10.5° as well as VAS increase with a mean value 45 mm{how would this effect spine height?}. The erector spinae was active in a larger angle during flexion as well as extension after trunk axial twisting.”<-creep implies a change in shape but whether that change involved a longitudinal increase is unclear.
“the elastic forces generated by the passive component of muscles are the main sources of passive resistance at the initial twisting motion, and then toward the end of ROM lumbar posterior ligaments and IVD will start to generate elastic forces and become the main contributor. This finding suggests that prolonged trunk axial twisting could also generate passive tissue creep and cause an alternation in the synergy between lumbar active and passive tissues.”
” The shear forces and moment created by spinal twisting within discs might elicit a shrinkage on spine by making the nucleus pulposus loose some fluid just like twisting a cloth full of water.”<-however this could also make the spine adapt by developing methods to absorb and retain more water.
Here’s a look of individual IVD cells response to loading regimes:
Region specific response of intervertebral disc cells to complex dynamic loading: an organ culture study using a dynamic torsion-compression bioreactor.
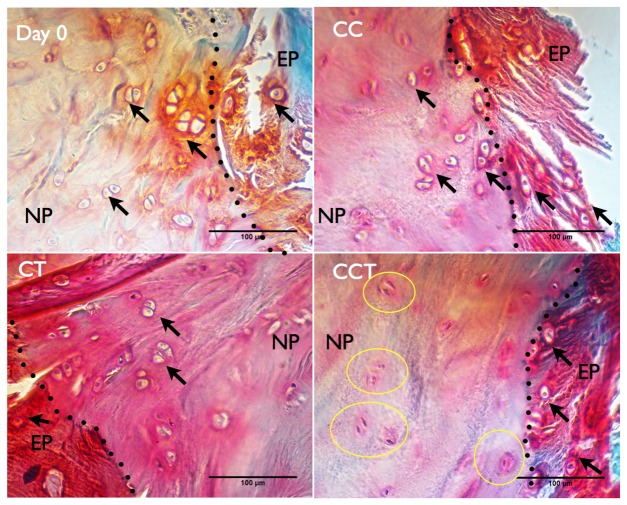
“We applied four different loading modalities [1. control: no loading (NL), 2. cyclic compression (CC), 3. cyclic torsion (CT), and 4. combined cyclic compression and torsion (CCT)] on bovine caudal disc explants”<-combined torsion and compression would be most akin to stretching as when you stretch one way you’re compressing another.
“In the CCT group, less than 10% nucleus pulposus (NP) cells survived the 14 days of loading, while cell viabilities were maintained above 70% in the NP of all the other three groups and in the annulus fibrosus (AF) of all the groups.”
“Gene expression analysis revealed a strong up-regulation in matrix genes and matrix remodeling genes in the AF of the CCT group”<-maybe developed of the extracellular matrix could increase height?
“Daily cyclic loading is important for disc health, as it assists in the transport of large soluble factors across the disc and from its surrounding vascular supply and applies a direct and indirect stimulus to disc cells.”<-This would increase height but does stretching apply a stimuli further than that?
” Characteristics of DD include increased cell death, a decrease in disc height due to a loss of essential matrix components which can also be reflected by an increased matrix catabolic gene expression (MMP-3, MMP-13, ADAMTS-4) but decreased anabolic gene expression (collagens and proteoglycans), increased inflammatory response (TNF-a, IL-1b, IL-6) and changes of mechanical properties of the disc (increased stiffness)”<-Although some of these things could also be involved in a anabolic protocol but the main thing we should watch is loss of essential matrix components in terms of reducing height.
“During the day, the disc experiences a pressure range from 0.1–1.1 MPa . However, studies have shown that dynamic compressive loading of >0.8 MPa could induce early DD; dynamic loading of physiological magnitude (1 MPa) at a frequency of 0.2 Hz was suggested to be the best in preserving disc metabolism while a frequency of 0.01 or 1 Hz could stimulate catabolic gene expressions ; signs of mild disc degeneration were seen when loading was applied in a longer term of 8 weeks (8 h/day) even at a physiological magnitude (1 MPa). The complex loading of side bending (in the form of asymmetric compression) and cyclic compression induced a greater structural disruption to the disc than simple cyclic compression”<-This would suggest that the best way of being as tall as possible would be to avoid excessive stimulus.
” torsional[twisting] injury is one of the initiators of disc degeneration, as evidenced by a decrease in disc height and a drop in disc proteoglycan content”<-so getting injured while stretching could possible reduce height.
“cyclic torsion could cause injury to the disc, provoking increased inflammatory (TNF-α and IL-1β ) and altered elastin gene expressions. An increase in elastin content in the AF is one of the observations in degenerated human discs and an alteration in the elastin fiber network might render the AF more susceptible to micro failure under torsion and bending”
“asymmetric dynamic compression (bending with compression) caused annulus fibrosus (AF) delamination and cell apoptosis”
“Discs used in this study had a mean dimension of 16.63±1.55 mm diameter and 9.58±1.22 mm height at day 0. By the end of the experiment, disc volume was increased by 10±5.76% for NL[no load], but increase in disc volume were less than 2% in all the other groups with loading”
“There was a slight increase in mean disc height of around 3% in the NL and CT[cyclic torsion/twisting] groups, while disc height was decreased by about 2% in the groups with cyclic compression (CC and CCT).”
“In the NP, collagen 1 expression was significantly up-regulated in CT. ADAMTS-4 was increased over 1000 fold in both CT and CCT, where its inhibitor TIMP-3 was also increased more than 10-fold”
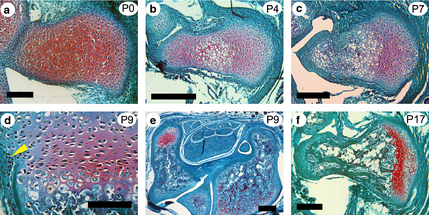
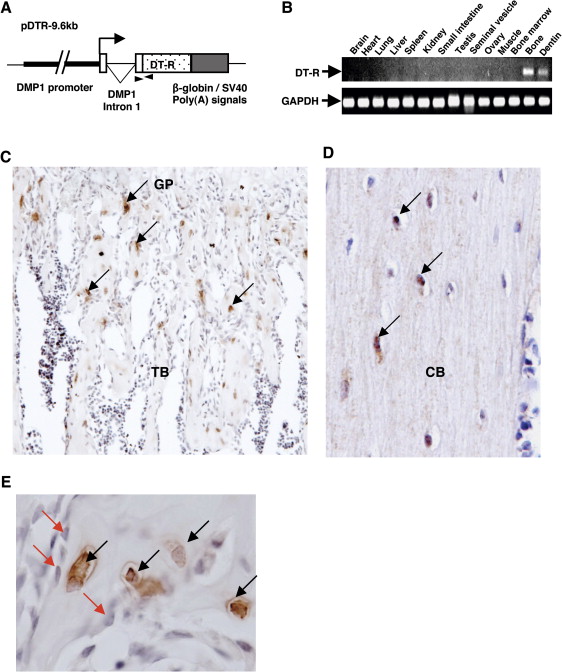
” In the transition zone between the cartilaginous endplates (EP) and the nucleus pulposus (NP) , cells stayed as chondrocyte-like cells (indicated by black arrows) in the CC and CT groups with a round cell nucleus surrounded by lacunae. However, in CCT, very few cells stayed as chondrocyte-like cells in the cartilaginous endplate and cells right across the endplate region changed to spindle-shaped and the cell lacunae and the cell boundary were lost.”<-This could be a key to height growth. Maybe one way to restore growth plate is to remove either compressive or torsion forces in the bone.
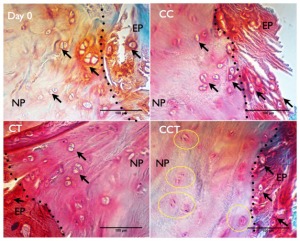 You can definitely see the loss of cartilage but is it an irreversible loss?
You can definitely see the loss of cartilage but is it an irreversible loss?
“torsion-compression loading has caused micro-damage to the collagen, therefore disc cells have been activated to compensate for the destruction. As shown in the gene expression result, groups with torsion (CT and CCT) showed a larger increase in both anabolic and catabolic gene expression by AF cells as compared to no loading or pure compression, indicating that AF cells were more sensitive to torsional loading stimulation. Therefore they responded by increasing some matrix production and matrix destruction enzymes to remodel the matrix environment.”
“One possible reason for the difference in response between the NP and AF to the same loading is due to the fundamental difference in the matrix component and structure between NP and AF. AF collagen fibers are aligned in an angle that can withstand shear force but the disorganized gel-like matrix of the NP cannot withstand a high shear force under combined compression and torsion. The NP, which is mainly composed of water, proteoglycans and collagen 2, is more resistant to compressive force than direct shear force as in compression and torsional load. A uniform torque applied to the disc will result in a hoop strain within the tissue, which increases with the distance from the center of rotation. It might be that the reaction of the annulus cells to the applied torsion stress is also different between the outer annulus and the inner annulus fibrosus as the inter-lamellar angle decreases radially from the periphery to the center from 60° towards 40°. Moreover, the elastic fiber arrangements in intra-lamellar and interlamellar zones were shown to be architecturally distinct, suggesting that they perform multiple functional roles within the AF matrix structural hierarchy”

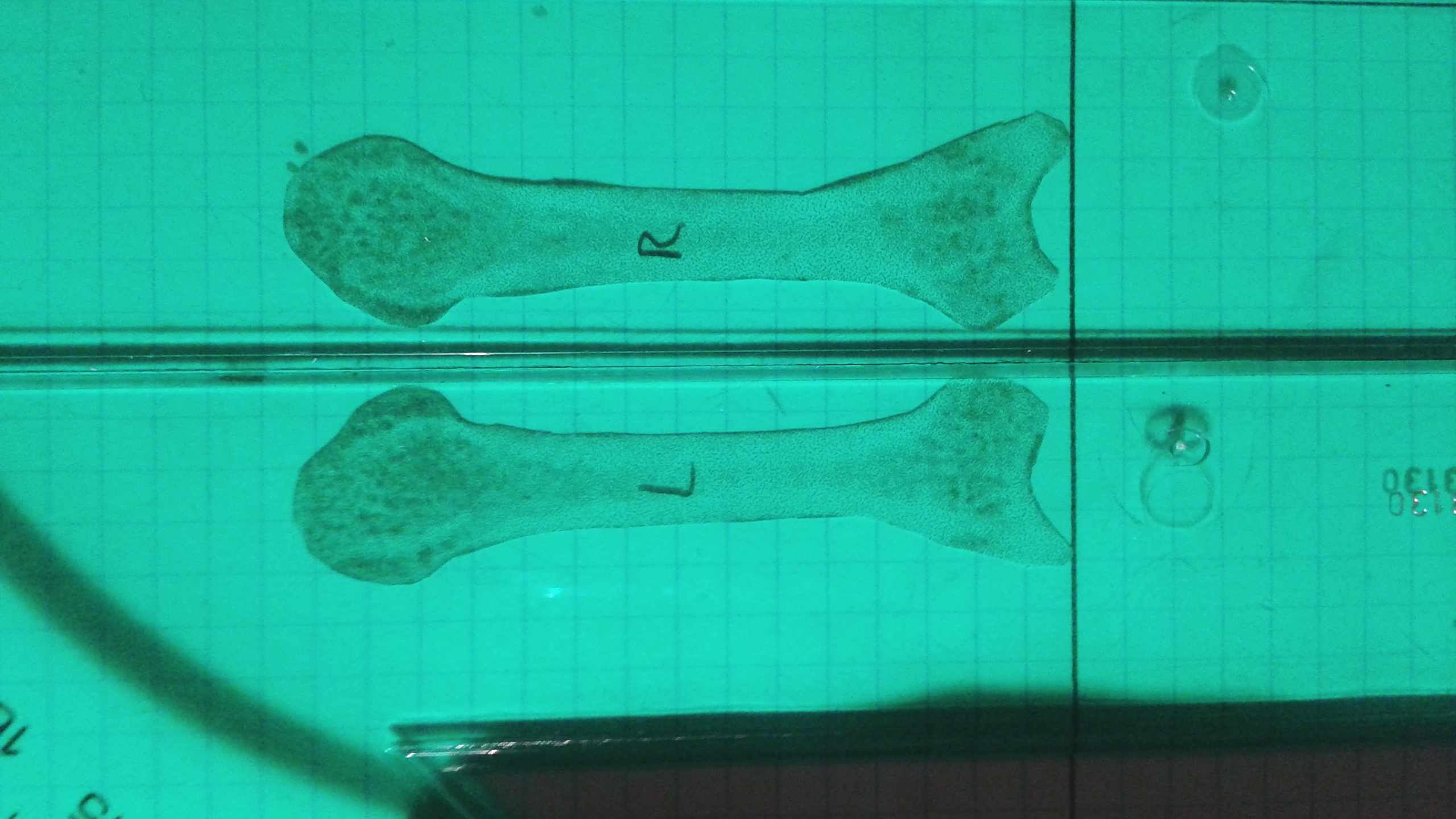
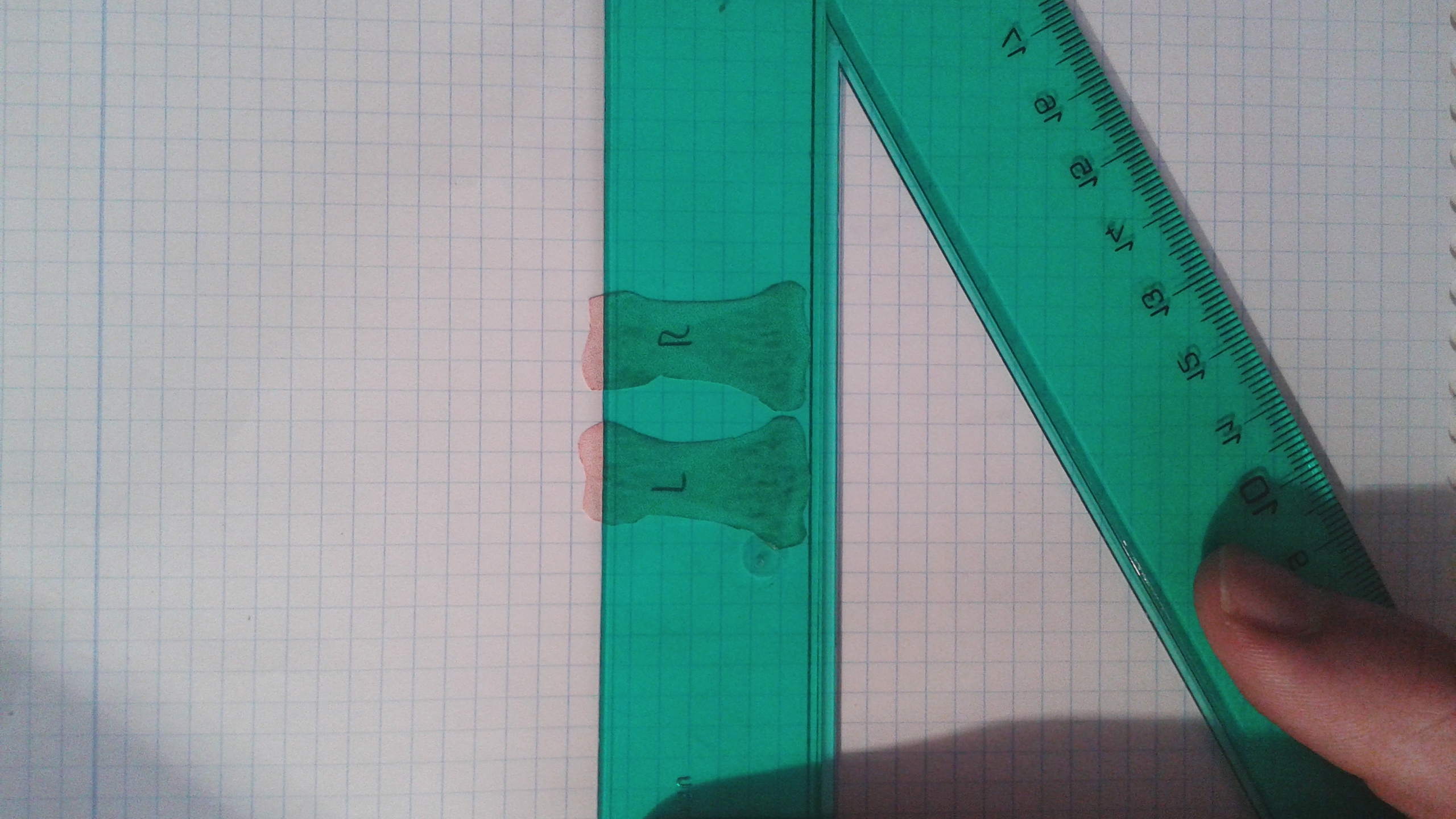
 This is a cut out of the proximal index fingers of the right and left finger bones from the x-ray from the link provided above. Click on the image as the image shows flipped for some reason. The right bone is the one labeled with the R. The measurements were done by adjusting the two bones until they were as long as possible. This insures that both bones were given the same advantages and the angle at which I put my finger is not a factor. Measurements were done by someone else.
This is a cut out of the proximal index fingers of the right and left finger bones from the x-ray from the link provided above. Click on the image as the image shows flipped for some reason. The right bone is the one labeled with the R. The measurements were done by adjusting the two bones until they were as long as possible. This insures that both bones were given the same advantages and the angle at which I put my finger is not a factor. Measurements were done by someone else. This one slopes to the right only at about .80 degrees(measuring the straight line downwards it is .80 off from 90 degrees. This images slope favors the right as well but not nearly as much. The left bone is longer.
This one slopes to the right only at about .80 degrees(measuring the straight line downwards it is .80 off from 90 degrees. This images slope favors the right as well but not nearly as much. The left bone is longer.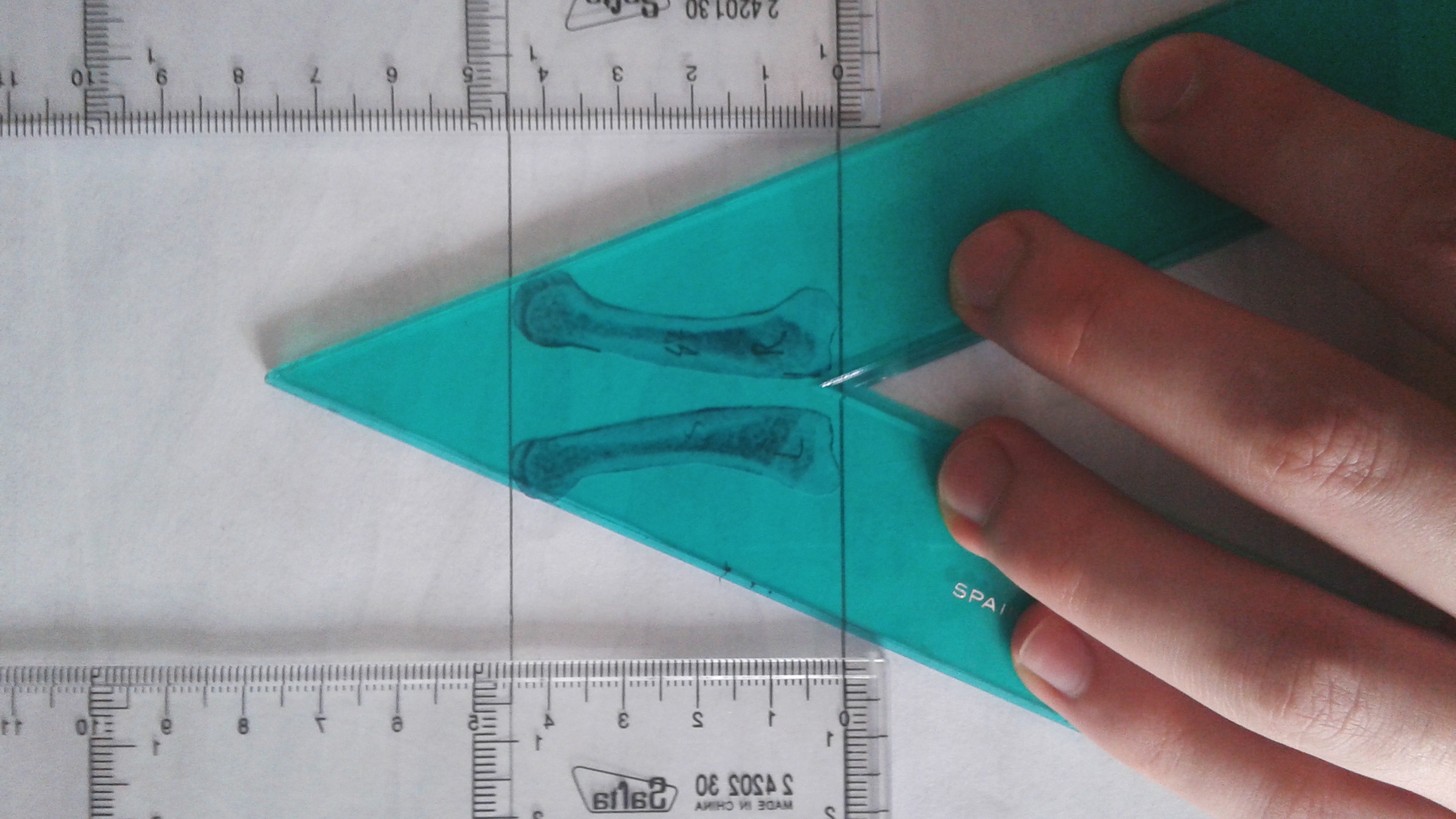 You can see here the the epiphysis of the right index finger are much larger but the left finger is longer overall.
You can see here the the epiphysis of the right index finger are much larger but the left finger is longer overall.